
In last year’s report we opted for a narrow approach to the Regional Profiles section, focusing only on Sub-Saharan Africa and the 15 countries in the region that had finalized their FP2030 commitments by August 2022. This year, with commitments in hand from every region with an FP2030 hub — Asia and Pacific (AP); East and Southern Africa (ESA); North, West, and Central Africa (NWCA); and Latin America and the Caribbean (LAC) — we expand our scope to include all four regions.
Our focus this year is postpartum family planning, a topic chosen specifically by the Regional Hubs. In 2023 there were more than 95 million births in low- and lower-middle income countries, and 59 million births were unintended.4 Additionally, more than 80% of births to the youngest mothers (under the age of 20) occur in these countries. Postpartum family planning is a high impact practice with demonstrated ability to improve maternal and newborn health outcomes and increase the uptake of contraception.
Each regional section begins with a demographic update on the population of women of reproductive age (WRA), changes over time to this population, the total fertility rate (TFR), total number of births, median age of the population, modern contraceptive use, and most common methods used in region. All demographic data is sourced from the United Nations Population Division.

We next summarize the results of the Gender Equality and Social Inclusion Assessment (GESI) for the region, where available. The gender assessment process began in 2023 with the ESA and NWCA hubs, and is continuing in 2024 with the AP hub. (The LAC hub has not yet initiated the process.) The gender assessments provide a framing context for the region, highlighting how gender norms and policies influence family planning at the individual, household, community, and societal level.
While gender norms and laws affect women and girls throughout their lives, the impacts are perhaps most profound in relation to pregnancy. Women’s physical, emotional, and financial wellbeing throughout the pregnancy continuum — from prenatal to postpartum — are heavily shaped by gendered expectations and limitations.
In our data analysis, we review postpartum family planning use in the context of pregnancy risk and spacing between births (birth intervals) using Demographic Health Surveys. We analyze the extent to which postpartum modern contraceptive use5 differs based on place of delivery, the age of the mother, and whether she was married or not when she had her first child. We also explore health systems-level indicators, such as the timing of postnatal checks and the content of these postnatal checks, to identify patterns and suggest opportunities for improvement.
While this analysis focuses on counseling and uptake during the postpartum period, family planning options should be discussed with women during antenatal visits as well. The World Health Organization recommends a minimum of eight antenatal contacts, which should include discussion of postnatal family planning options along with other critical health concerns.6
Prompt postnatal checks are critical. Women in the first postpartum weeks have little risk of pregnancy, but this is a critical window for counseling on family planning. It is a time when women are in contact with health providers for essential services, and every touchpoint is an opportunity to ensure that their contraceptive needs are being met. Too many women are unprepared for the return of fertility because family planning was not offered postpartum. Women should be counseled on all the contraceptive options available to them, including methods that can be initiated immediately after delivery. Early counseling is strongly correlated with higher uptake of contraception.
In our analysis we found that in every region and every country (with the sole exception of Cambodia), MCP is higher for women who received their postnatal checks within 4 hours of delivery compared to women who received their postnatal checks at 41+ days or never. (We use 4 hours after delivery as a proxy for how attentive the health care system is to women’s needs; our assumption is that a 4 hour check implies that subsequent checks are also happening appropriately. The World Health Organization recommends that counseling on family planning be offered within the first 24 hours of delivery and beyond.7) Prompt postnatal care varies greatly by region: in ESA, the majority of women do not receive a postnatal check within 4 hours of delivery; in NCWA, at least a third of women do; and in AP, the majority of women receive these checks.
The place of delivery should not determine the types of services women are receiving. Women who give birth at home consistently have lower MCP in the postpartum period. Some countries also show a difference in postpartum MCP depending on whether the births took place in public or private health facilities. This could indicate gaps in the services being provided. For home births, the World Health Organization recommends that the first postnatal contact should be as early as possible within 24 hours of delivery.8 If contraceptives are offered through community-based distribution, health workers should ensure that the new mother is visited promptly and provided with postpartum family planning options. Public or private health facilities with a track record of lower contraceptive uptake may need to revamp their postpartum counseling and services.
Regardless of a woman’s age, tailored counseling and services should be provided. Postpartum contraceptive uptake differs by age in several countries. In some countries, the youngest mothers — those under the age of 20 — are being left behind; in other countries those 35 or older are being left behind. Biologically, the youngest mothers have the highest risk of becoming pregnant again, while those over 35 are at higher risk for pregnancy-related complications. To ensure that they are able to make informed choices about their health, postpartum women of all ages should be counseled and provided services.
Differences in contraceptive use by marital status and age should be explored as possible signals of gender-based barriers. In several countries, postpartum MCP is higher among women who gave birth outside of marriage than those who gave birth within marriage; this could point to married women having less autonomy in decision-making.9 In countries where postpartum MCP is lower among women who gave birth outside of marriage, this could be an indicator that family planning services are not readily available for unmarried women (who also tend to be younger).10 These are possibilities that should be investigated to ensure that women are not being excluded from making decisions about their own health.
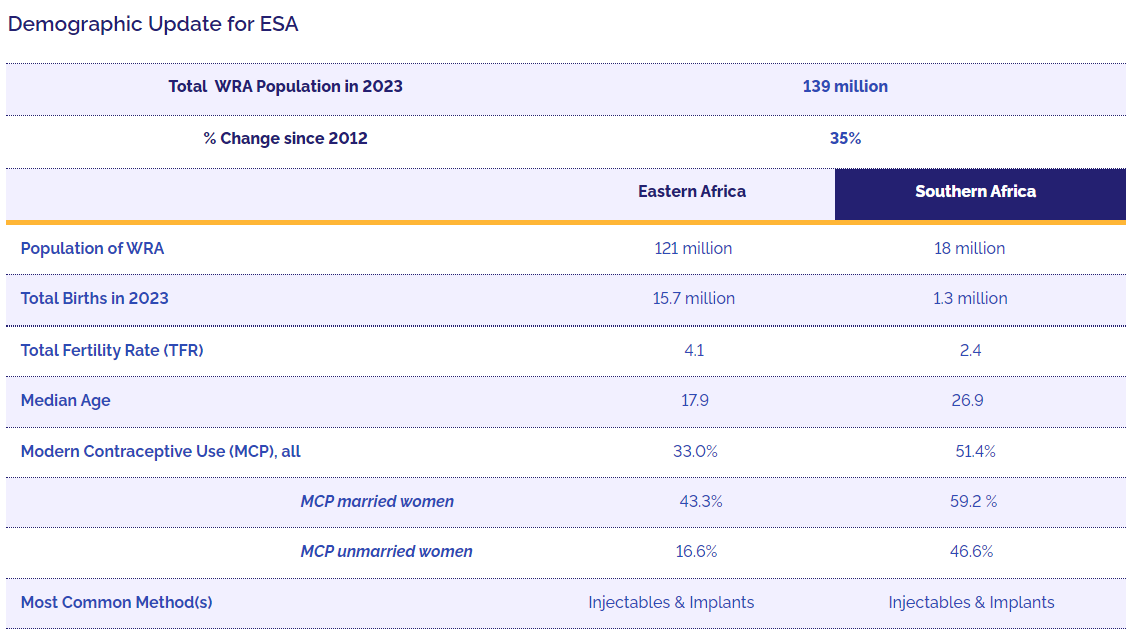
East and Southern Africa has the fastest-growing population in the world. The number of WRA (women of reproductive age) rose by 35% between 2012 and 2023 — from 102 million to 139 million. Almost four million women reached reproductive age just in the past year (from 2022 to 2023).
Total WRA Population in 2023
139 million
% Change since 2012
35%
Eastern Africa
Southern Africa
Population of WRA
121 million
18 million
Total Births in 2023
15.7 million
1.3 million
Total Fertility Rate (TFR)
4.1
2.4
Median Age
17.9
26.9
Modern Contraceptive Use (MCP), all
33.0%
51.4%
MCP married women
43.3%
59.2 %
MCP unmarried women
16.6%
46.6%
Most Common Method(s)
Injectables & Implants
Injectables & Implants
Countries in East and Southern Africa have been largely successful in adopting laws and policies to support family planning and SRHR. The Maputo Protocol has played a vital role in spurring domestic development of legal frameworks. Constitutions commonly include rights on accessing health, and both Rwanda and Zambia have adopted gender integration laws to shape government policies and programs.
But the region struggles with age of consent laws and policies when it comes to adolescents. Legal ambiguity concerning statutory rape and the minimum age for access to contraception affects service delivery. Other laws and policies — loopholes in child marriage laws, anti-LGBTQIA+ laws, and the absence of healthcare confidentiality provisions — also hinder access to family planning and other SRH care.

Gender norms in the region are enforced by strong sanctions and influenced by religion, culture, and traditions. Most ESA countries face issues revolving around adolescent girls’ sexuality: child marriage, teen pregnancy, and female genital mutilation. Norms that regard men as “head of the household” limit women’s autonomy and contribute to restrictions on SRHR for unmarried women and adolescents, while economic discrimination and exclusion perpetuate the lack of access to healthcare. Notable progress in political representation has been made in some countries, but discrimination still stifles women’s leadership in government and health workforces.
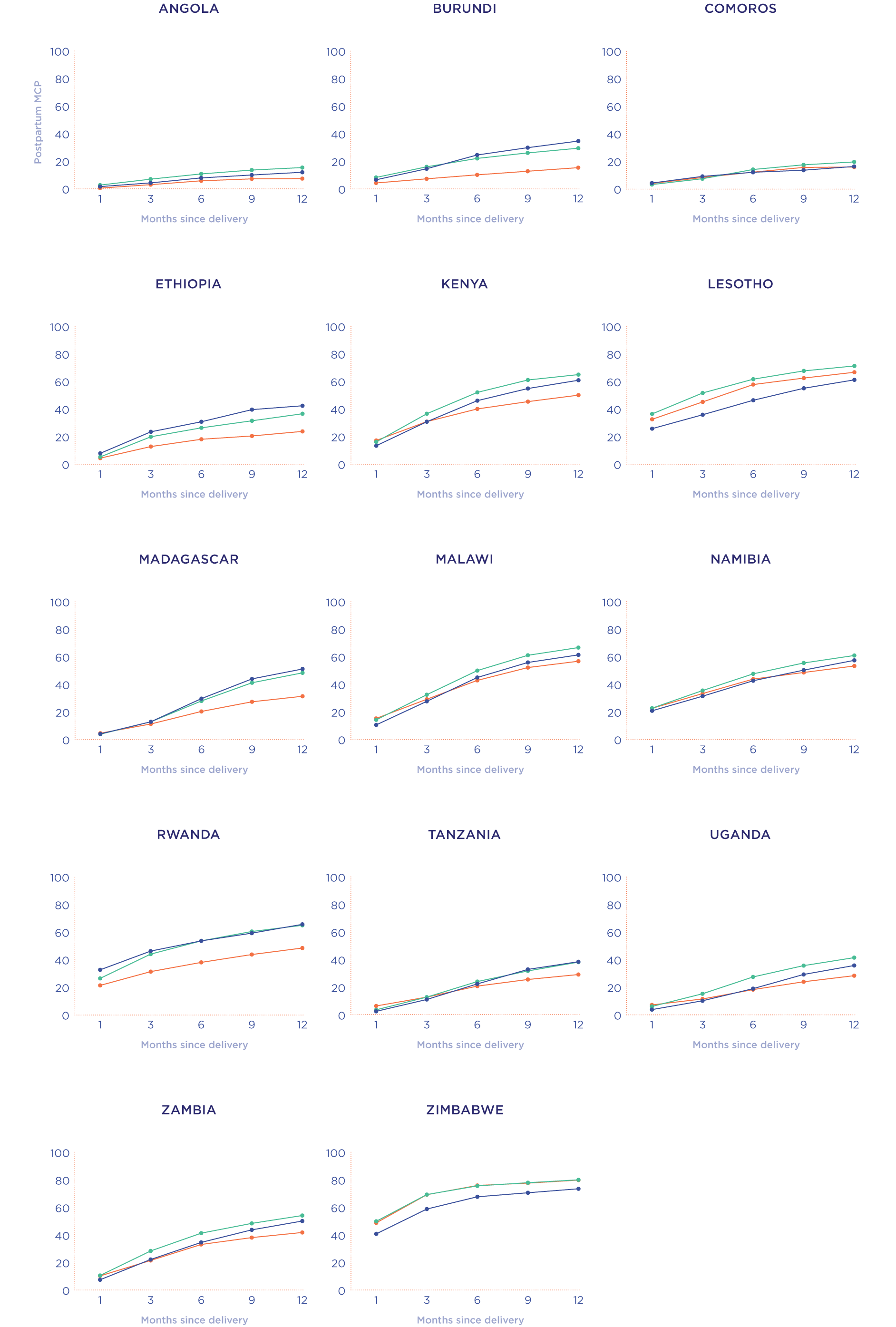
Countries reviewed: Angola, Burundi, Comoros, Ethiopia, Kenya, Lesotho, Madagascar, Malawi, Namibia, Rwanda, Tanzania, Uganda, Zambia, Zimbabwe
In 11 of the 14 countries we reviewed (all except Lesotho, Namibia, and Zimbabwe), MCP is low in the early postpartum period, which in this study we define as within 1 month of delivery. The risk of a pregnancy is low in this period because most women are postpartum insusceptible, meaning that they are either abstaining from sex or amenorrheic (not menstruating). Postpartum insusceptibility declines over time, but most women in ESA are still not at risk of a pregnancy at 6 months postpartum. But by 12 months postpartum, women in all countries except Angola, Burundi, Ethiopia, Malawi, and Rwanda have become susceptible to a pregnancy.
In all countries, MCP starts to increase as time since delivery increases. MCP at 1 month postpartum is highest in Zimbabwe at 48.3%, followed by Lesotho at 34.1% and Namibia at 22.1%. These are also countries with high MCP overall.
The World Health Organization recommends that births be spaced at least 24 months apart. In all 14 countries we reviewed, more than 10% of births are too closely spaced, falling within two years of a previous birth. And in five countries (Angola, Comoros, Ethiopia, Madagascar, and Uganda), more than 20% of births are too closely spaced. Closely spaced births are particularly high in Comoros, where nearly a third (30%) of pregnancies occur within a two-year interval. Very short birth intervals of 7-17 months — which are the riskiest — are not common in the region, although around 1 in 10 births in Angola, Comoros, and Madagascar do fall within this very close interval.
Facility Type: In all countries, women who delivered at home have the lowest MCP at all timepoints in the postpartum period. In some countries (Ethiopia, Kenya, Namibia, Rwanda, and Zimbabwe), the gap in MCP between women who delivered at home versus a facility (either private or public) is particularly wide and continues to widen until 12 months postpartum. By 12 months postpartum, the gap in use is at least 20 percentage points. This highlights the need for community-based distribution of contraceptives, with health workers who are trained in postpartum family planning and prepared to provide prompt, appropriate counseling and services.
Age of Mother at Most Recent Birth: In most of the countries we reviewed, postpartum MCP was lowest among the oldest mothers (those aged 35-49). Modern contraceptive use was broadly similar for mothers in the <20 age group and the 20-34 age group. In three countries — Burundi, Ethiopia, and Madagascar — MCP at 6 months postpartum was highest among the youngest mothers (those under age 20).
Marital Status of Mother at First Birth: In 7 of the 14 countries we reviewed (Comoros, Ethiopia, Kenya, Lesotho, Madagascar, Namibia, and Zambia) there is no real difference in postpartum contraceptive use among women who had their first child within marriage or outside of marriage. In Angola, Burundi, Rwanda, Tanzania, and Uganda, women whose first births were outside of marriage had higher modern contraceptive use at 6 months postpartum. Conversely, in Malawi and Zimbabwe, women whose first births were within marriage had higher modern contraceptive use at 6 months postpartum.
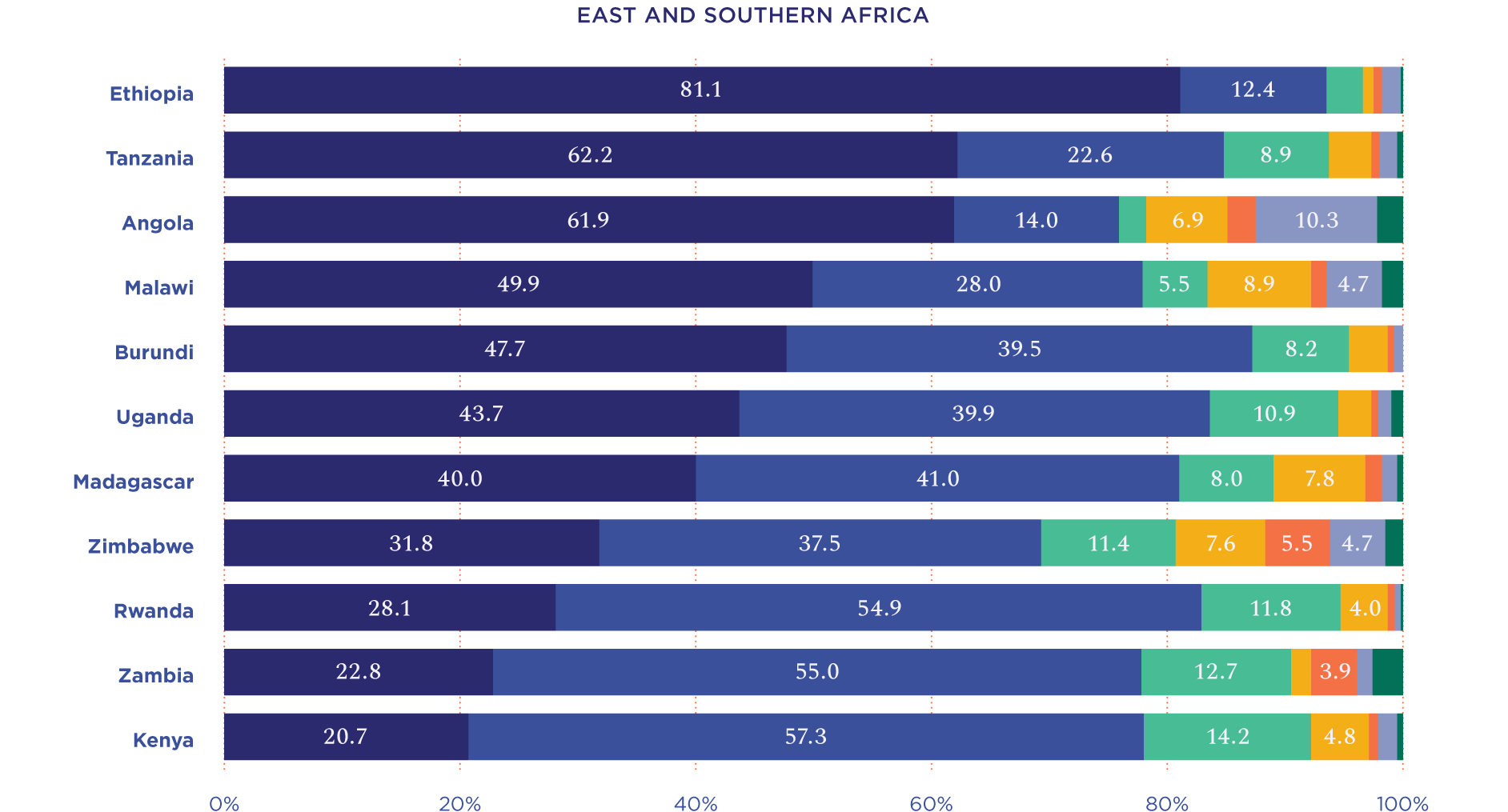
Ensure all mothers receive timely postnatal care. A significant percentage of women in every country we analyzed received their one and only postpartum check either 41+ days after delivery or not at all. This includes more than 80% of postpartum women in Ethiopia; more than 60% of postpartum women in Angola and Tanzania; more than 40% of women in Malawi, Burundi, Uganda, and Madagascar; and more than 20% of women in Zimbabwe, Rwanda, Zambia, and Kenya. Only in three countries — Kenya, Rwanda, and Zambia — do the majority of women receive their postnatal checks within 4 hours of delivery.
Strive to provide postnatal checks as soon after delivery as possible. In all countries, current MCP is higher for women who received their postnatal checks within 4 hours of delivery compared to women who received their postnatal checks at 41+days or never. The contrast is most pronounced for women in Angola (19.8% vs. 5.2%) and Ethiopia (45.5% vs. 25%). In some public health facilities women are discharged 12-24 hours after delivery, and they may not return for early postnatal checks unless there is a problem. Hence the importance of providing immediate postpartum care, including family planning counseling and options, while women are still in the facility.11
Ensure that postnatal checks include counseling on family planning that is tailored to the woman’s specific needs by age and marital status; young or unmarried women should not be denied services. While detailed information on the content of postnatal checks is scarce, the data we do have suggest that counseling on family planning may be missing in many encounters. In the latest household survey from Kenya (DHS 2022), which included questions on postnatal care, only 29% of postpartum women reported being counseled on family planning. In the most recent Service Provision Assessment from Tanzania (SPA 2014-2015), only 35% of antenatal care check-ups included information about postpartum family planning, while in Malawi’s most recent survey (SPA 2013-2014), only 12% of antenatal checks included this information.12
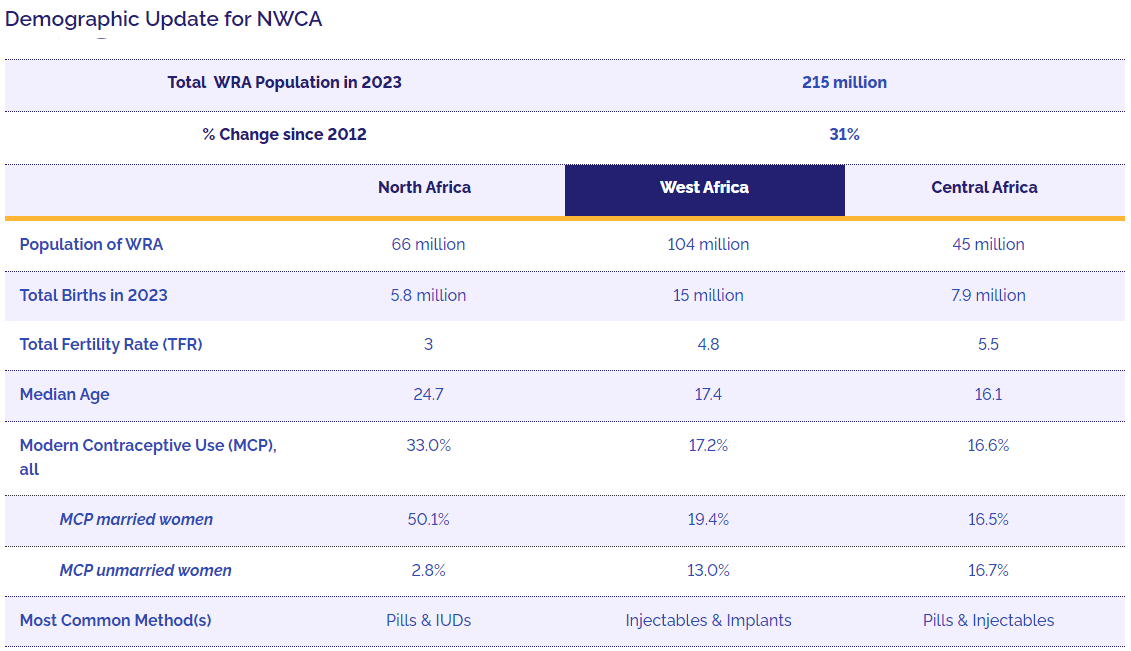
Central and West Africa have the highest fertility rates in the world, and Central Africa has the world’s youngest population, with half of its inhabitants aged 16 or under. Across the NWCA region as a whole, the population of WRA grew by 31% between 2012 and 2023: from 164 million to 216 million. Around 5.5 million women reached reproductive age just in the past year (from 2022 to 2023).
Total WRA Population in 2023
215 million
% Change since 2012
31%
North Africa
West Africa
Central Africa
Population of WRA
66 million
104 million
45 million
Total Births in 2023
5.8 million
15 million
7.9 million
Total Fertility Rate (TFR)
3
4.8
5.5
Median Age
24.7
17.4
16.1
Modern Contraceptive Use (MCP), all
33.0%
17.2%
16.6%
MCP married women
50.1%
19.4%
16.5%
MCP unmarried women
2.8%
13.0%
16.7%
Most Common Method(s)
Pills & IUDs
Injectables & Implants
Pills & Injectables

The GESI Assessment in this region focused on five countries: Benin, Burkina Faso, Côte d’Ivoire, Liberia, and Nigeria. The Maputo Protocol has been ratified in each country, and SRHR is guaranteed by law in every country except Côte d’Ivoire. The three Francophone countries are members of the Ouagadougou Partnership, which has galvanized the movement for family planning in West Africa. Liberia and Nigeria have also made political progress: Liberia has been a leader in inter-ministerial cooperation on gender and family planning, and in Nigeria the participation of civil society has led to an exceptionally strong national gender policy. But political battles over costs mean that family planning is not included in every country’s Universal Health Coverage plan.
Gender norms in the Francophone and Anglophone countries are similar, influenced by religion and tradition. Men dominate households and decision making on family size and health care access; adolescent girls’ sexuality is stigmatized. Adolescent access to contraception and sex education is hindered by social norms and lack of training of health workers. Policies guarantee access to school post-pregnancy, but implementation is blocked by stigma and discrimination. Child marriage in the region is high.
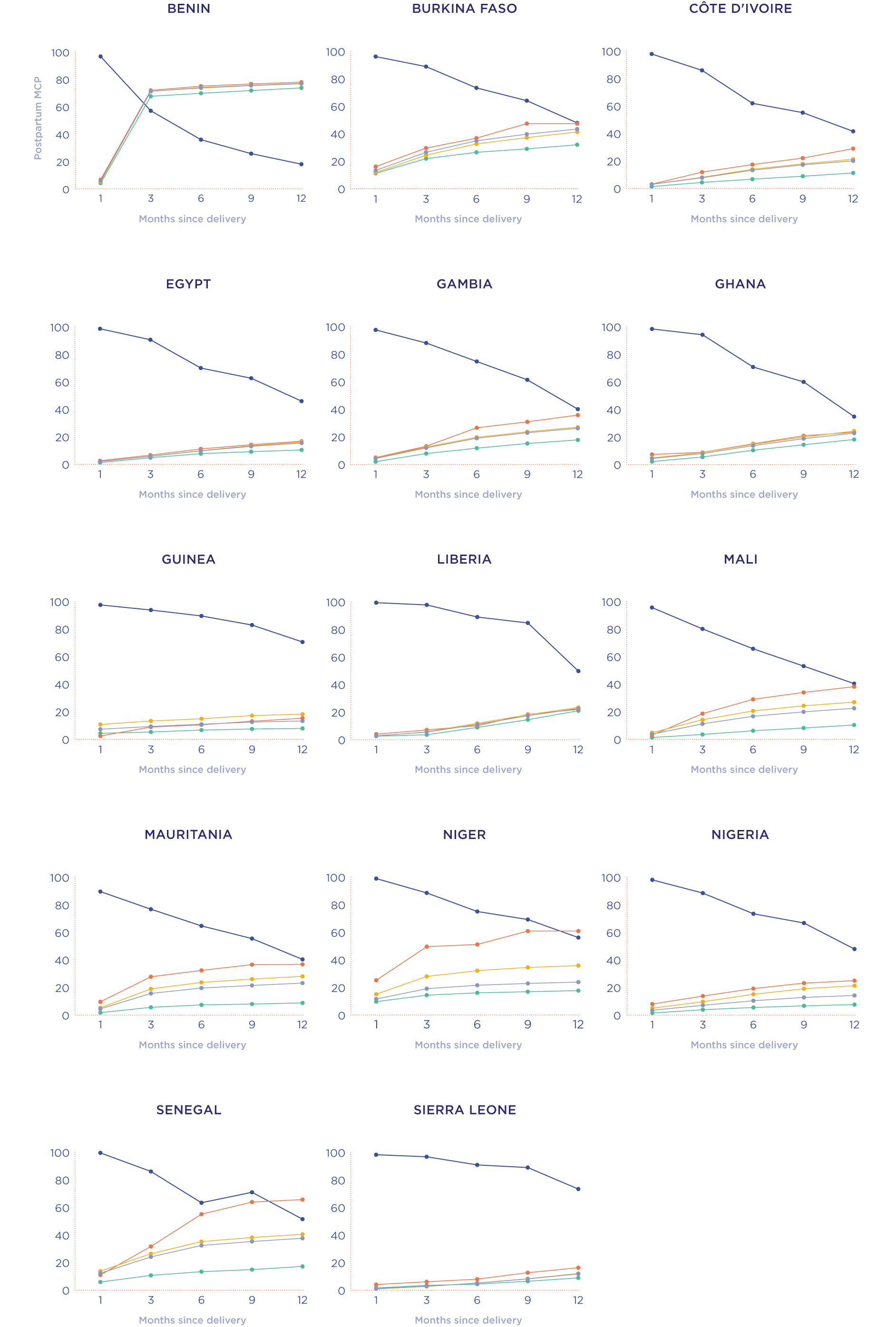
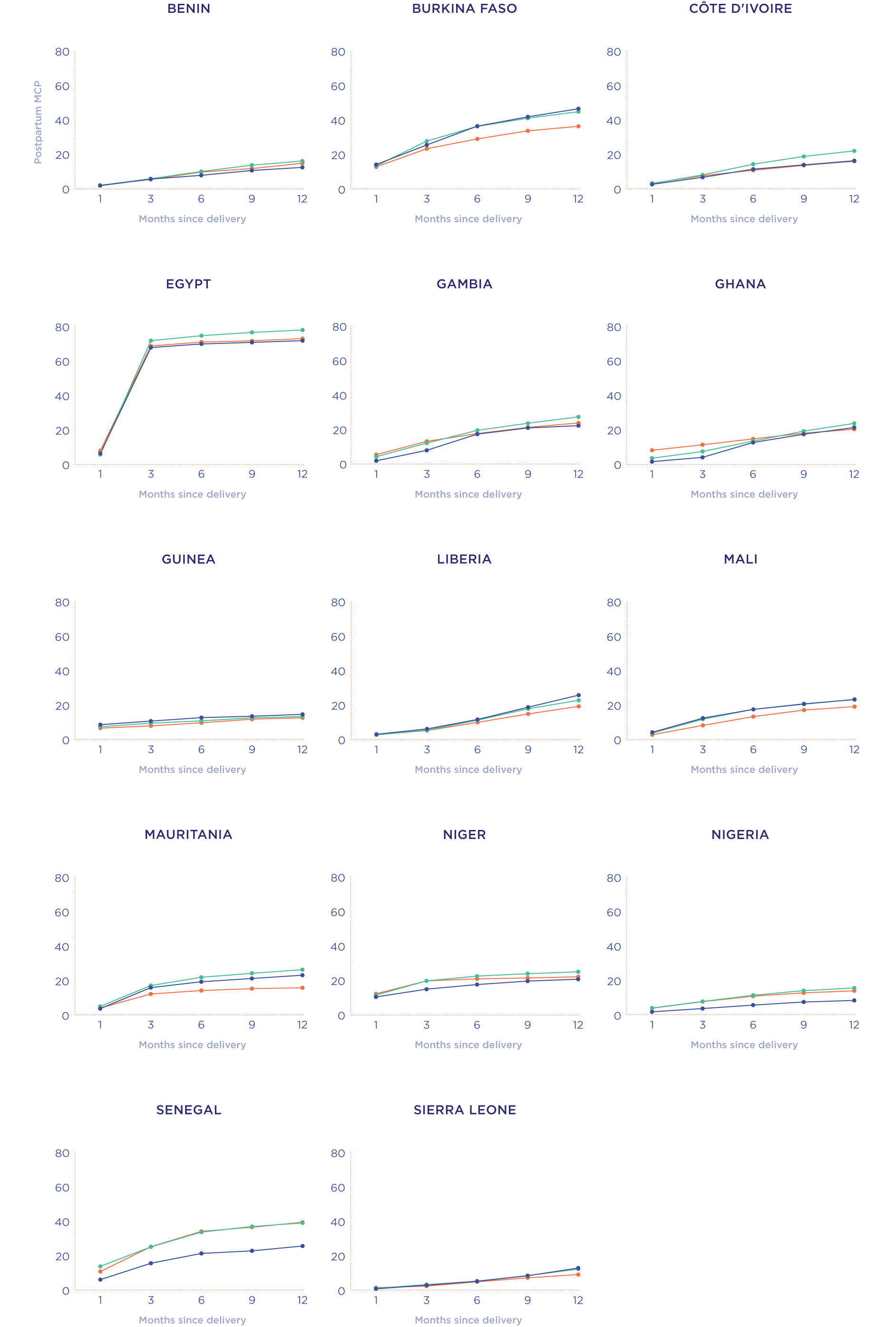
Countries reviewed: Benin, Burkina Faso, Côte d’Ivoire, Egypt, Gambia, Ghana, Guinea, Liberia, Mali, Mauritania, Niger, Nigeria, Senegal, Sierra Leone
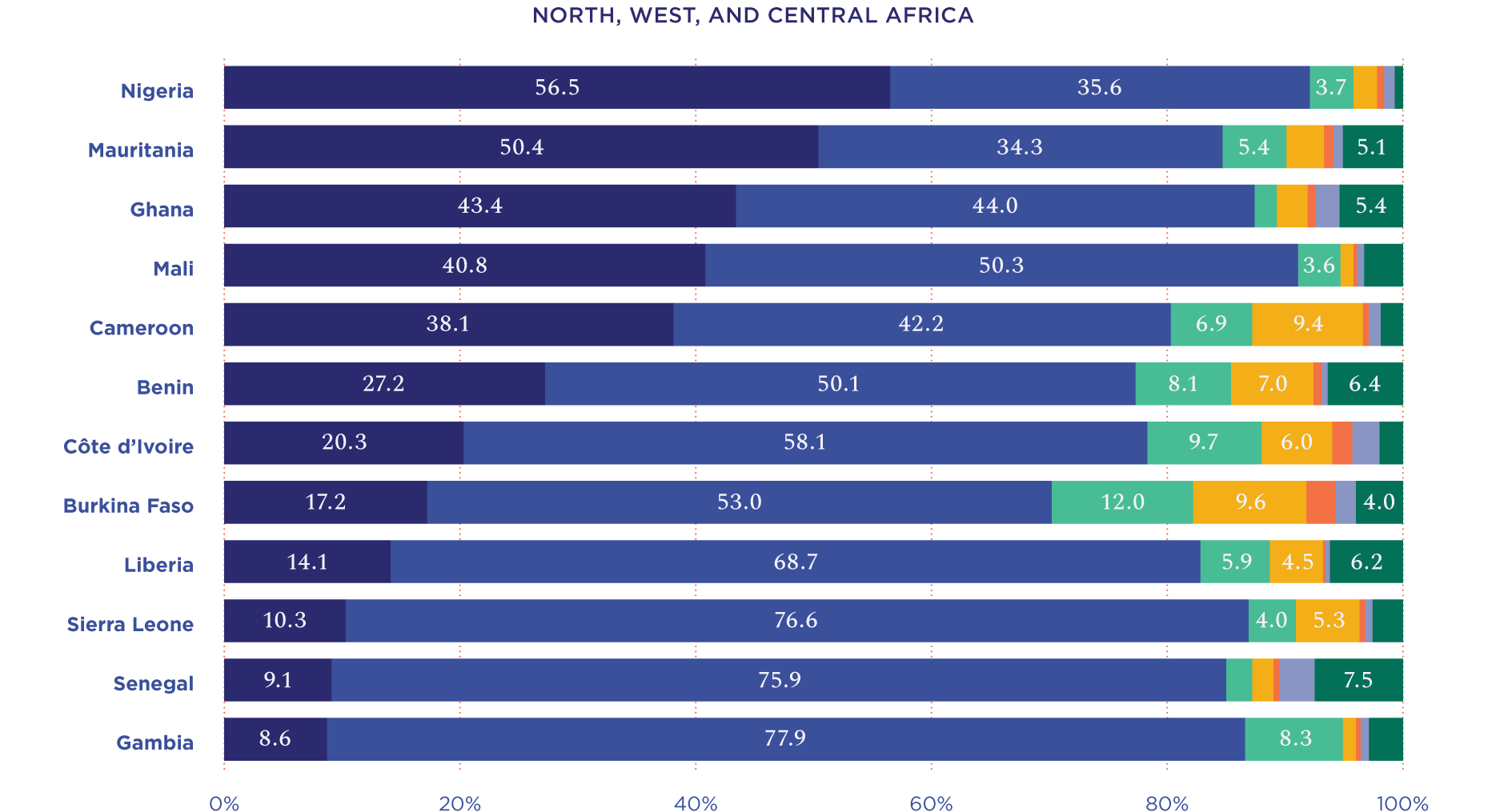
Throughout the region, postpartum use of modern contraception is extremely low in the early postpartum period; in most countries MCP at 1 month postpartum is 10% or lower. Postpartum insusceptibility is correspondingly high: 85% or higher at 3 months postpartum in every country except Egypt, where it’s 57%. At that point insusceptibility begins to decline steeply, and by 9 months postpartum, at least a third or more women are susceptible to a pregnancy. And by 12 months, a majority of postpartum women in all countries (except Guinea, Niger, Senegal, and Sierra Leone) are susceptible.
In all 14 countries of our study, more than 10% of births occurred within 24 months of a previous birth — closer than the WHO recommended spacing. In five countries (Cameroon, Mali, Mauritania, Niger, and Nigeria) the figure rises to 20%: one in five births are too closely spaced.
Facility Type: Women who deliver at home have the lowest modern contraceptive uptake in the postpartum period. The gap is widest in Senegal, where more than 1 in 4 women who deliver in a facility (public or private) are using a modern method at 3 months postpartum, while only around 1 in 10 women who delivered at home are using a modern method at that point. In six countries (Gambia, Mali, Mauritania, Niger, Nigeria, and Senegal) there is also a notable difference based on the type of facility, with MCP higher among women who delivered in a private facility rather than public. The difference is largest in Senegal: at 6 months postpartum, 55.1% of women who delivered in a private facility are using a modern method, compared to 35.2% of women who delivered in a public facility. The difference between public and private facilities in modern contraceptive uptake is more variable in NWCA than in ESA or Asia, with especially sharp differentials in Niger and Senegal.
Age of Mother at Most Recent Birth: In Benin, Gambia, Niger, Nigeria, and Senegal, the youngest mothers (those under age 20) are the least likely to be using modern methods at 6 and 12 months postpartum. The largest gaps in use between younger and older mothers are in Senegal and Nigeria. In Nigeria, only 5% of mothers in the <20 age group are using modern contraception at 6 months postpartum, compared to 11% of mothers aged 20-34. In Senegal, 21% of mothers in the <20 age group are using modern contraception at 6 months, compared to 34% of mothers aged 20-34. These gaps persist throughout the postpartum period. A different pattern obtains in Burkina Faso, Guinea, Liberia, Mali, Mauritania, and Sierra Leone, where the oldest mothers (those aged 35-49) have the lowest postpartum use of modern contraception.
Marital Status of Mother at First Birth: In all countries except Niger and Egypt, modern contraceptive use is higher among women who had their first child outside of marriage. This is especially pronounced in Mali. In Niger and Egypt, on the other hand, women whose first births were outside of marriage are less likely to use modern contraceptive methods in the postpartum period.
Identify and reach those women and girls who are not receiving postnatal care. Unlike the ESA region, in NWCA at least one-third of all postpartum women in all countries receive a postnatal check within 4 hours of delivery. This rises to more than 50% of women in Benin, Burkina Faso, Cote d’Ivoire, Gambia, Mali, Liberia, Senegal, and Sierra Leone. Conversely, more than half of postpartum women in Nigeria and Mauritania do not receive a postnatal check until 41+ days after delivery or never. Countries in the region should capitalize on their already-strong postnatal programs to identify why some women and girls are being left behind and develop tailored strategies to ensure they receive postnatal care.
Strive to provide postnatal checks as soon after delivery as possible. In all countries, current MCP is higher for women who received their postnatal checks within 4 hours of delivery compared to women who received their postnatal checks at 41+days or never. The contrast is most pronounced for women in Burkina Faso (35.8% vs. 27.8%) and Senegal (29.7% vs. 12.8%). Senegal also had the widest gaps between modern contraceptive use uptake between women who delivered at home versus in a facility.
Ensure that postnatal checks include counseling on birth spacing and family planning. Young or unmarried women should not be denied services. In the most recent Service Provision Assessment from the Democratic Republic of Congo (SPA 2017-2018), only 11% of antenatal consultations included information about postpartum family planning.13 This is the only relatively recent survey from the region.
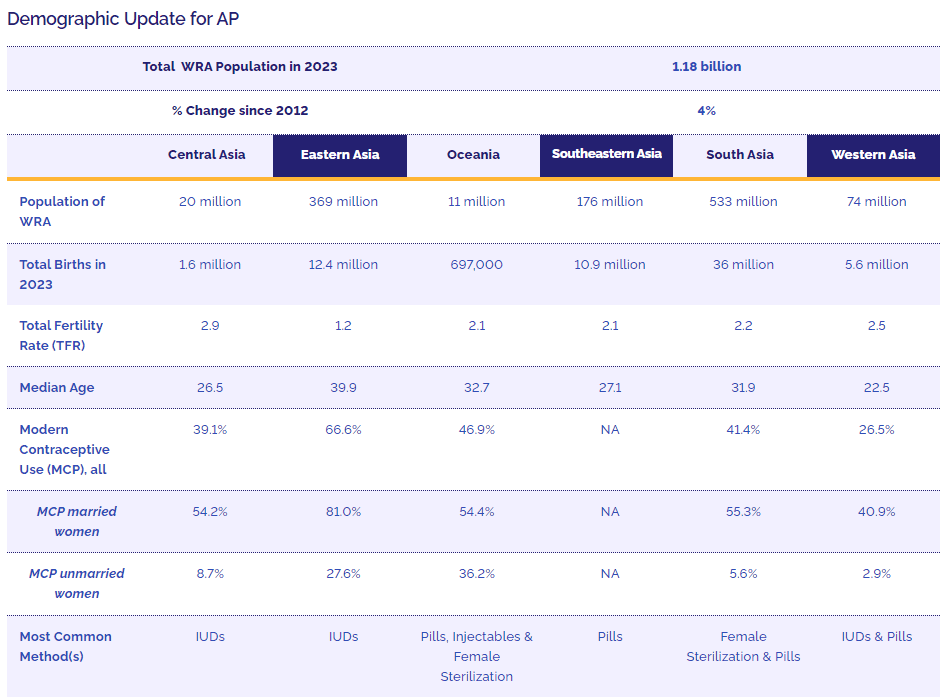
The AP region has the largest population in the world, but it is not growing as fast as the population of Sub-Saharan Africa. Nevertheless, the sheer size of the region’s population means that small percentage increases translate into very large absolute numbers. Between 2012 and 2023, AP added 40,000,000 million women of reproductive age. The fertility rate for the region as a whole is 1.9 —which is below replacement level.
Total WRA Population in 2023
1.18 billion
% Change since 2012
4%
Central Asia
Eastern Asia
Oceania
Southeastern Asia
South Asia
Western Asia
Population of WRA
20 million
369 million
11 million
176 million
533 million
74 million
Total Births in 2023
1.6 million
12.4 million
697,000
10.9 million
36 million
5.6 million
Total Fertility Rate (TFR)
2.9
1.2
2.1
2.1
2.2
2.5
Median Age
26.5
39.9
32.7
27.1
31.9
22.5
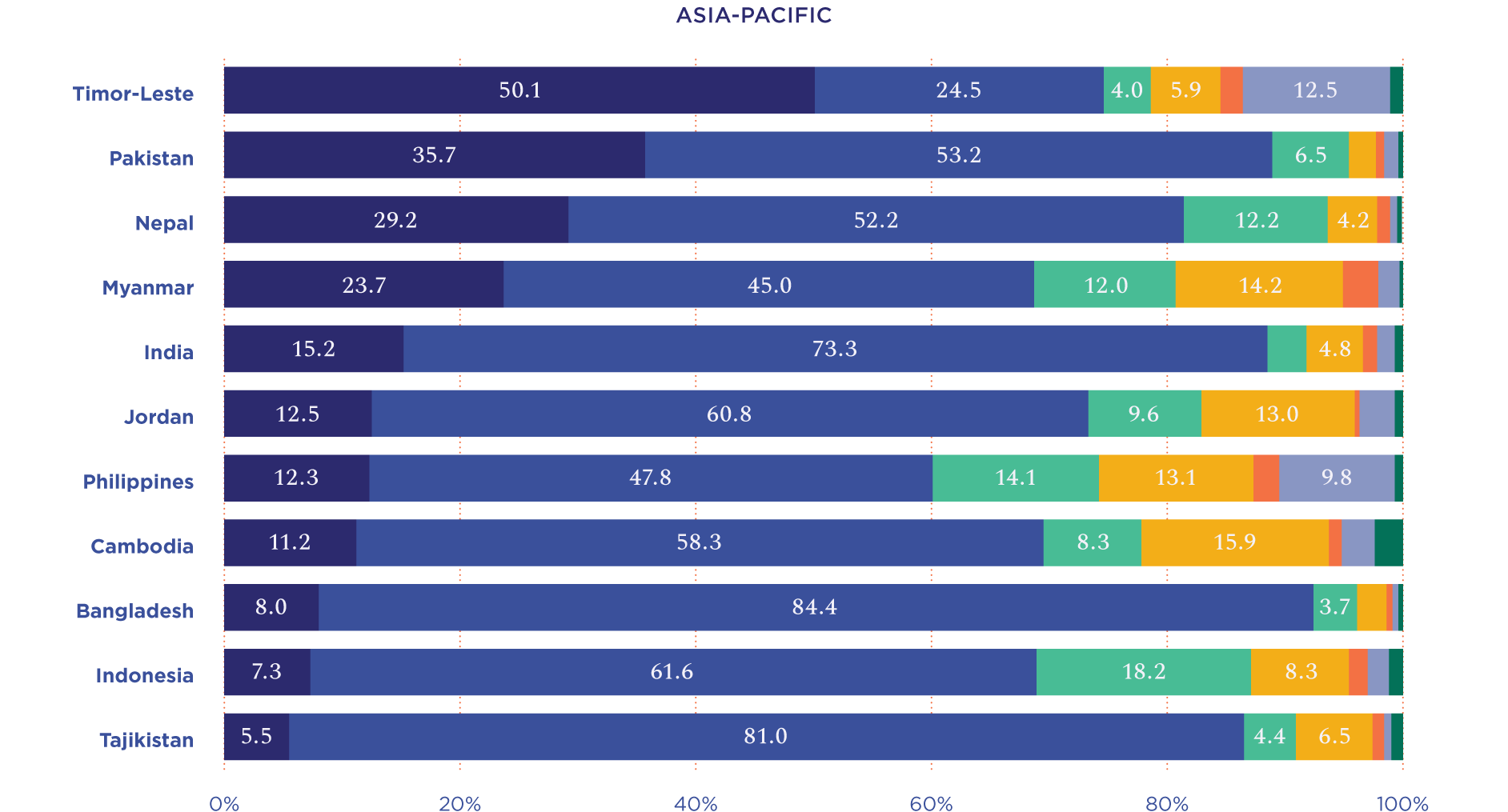
Modern Contraceptive Use (MCP), all
39.1%
66.6%
46.9%
NA
41.4%
26.5%
MCP married women
54.2%
81.0%
54.4%
NA
55.3%
40.9%
MCP unmarried women
8.7%
27.6%
36.2%
NA
5.6%
2.9%
Most Common Method(s)
IUDs
IUDs
Pills, Injectables & Female Sterilization
Pills
Female Sterilization & Pills
IUDs & Pills
Countries reviewed: Afghanistan, Bangladesh, Cambodia, India, Indonesia, Jordan, Kyrgyz Republic, Myanmar, Nepal, Philippines, Pakistan, Tajikistan, Timor-Leste, Yemen
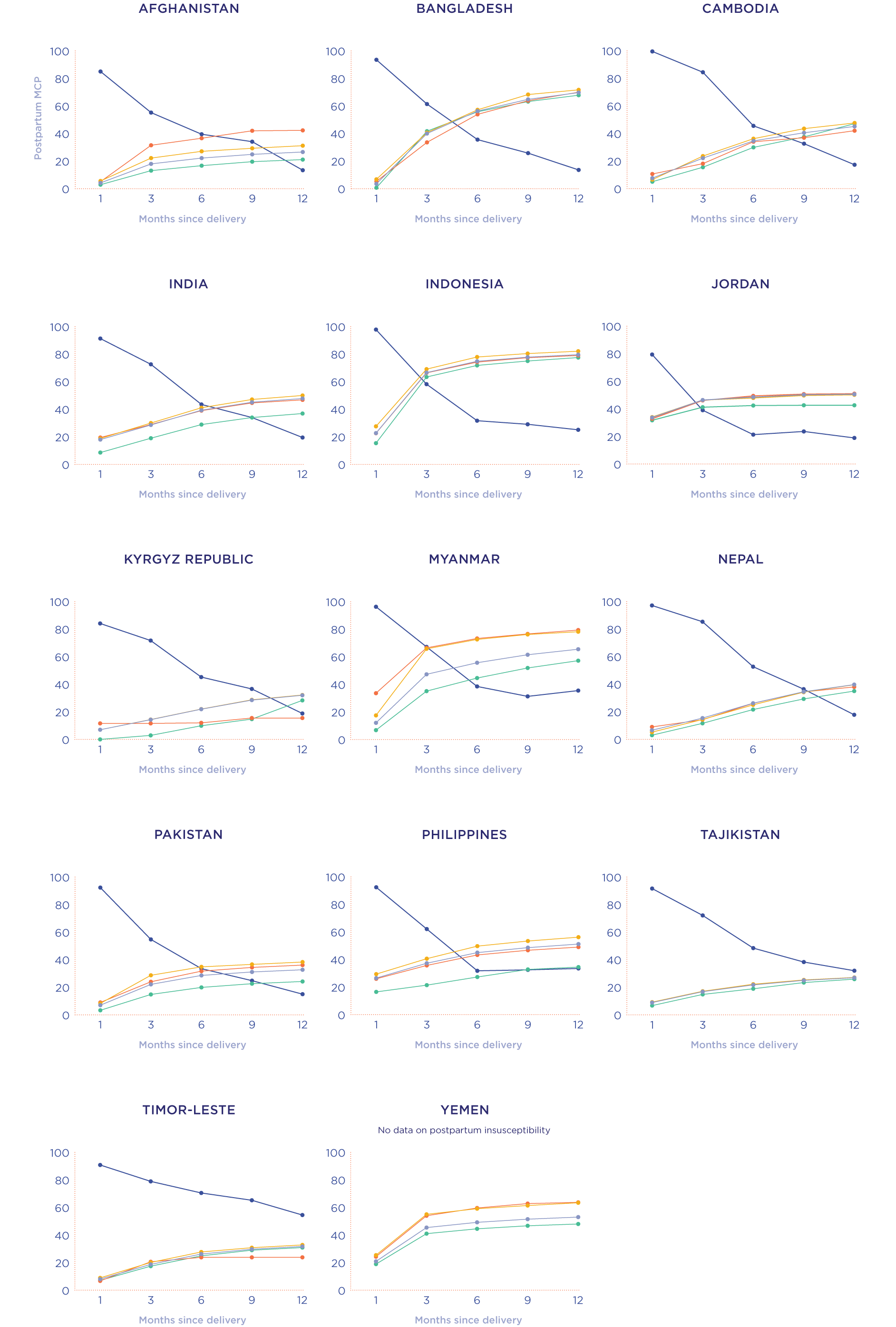
In most of the countries we reviewed, MCP is low in the early postpartum period (within 1 month of delivery); this is also when women’s risk of pregnancy is low due to postpartum insusceptibility. MCP increases in all countries as time since delivery increases. MCP use at 1 month postpartum was above 20% in Indonesia, Jordan, Philippines, and Yemen. MCP at 1 month is highest in Jordan at 33.7%, which could indicate immediate postpartum use since IUDS are the most common method in that country.
Postpartum insusceptibility declines more quickly than in the NWCA and ESA regions, with women in most AP countries becoming susceptible to a pregnancy at 6 months postpartum. Only in Nepal and Timor-Leste are most women still postpartum insusceptible at 6 months (52.7% and 70.5%, respectively). By 12 months postpartum, most women in all countries except Timor-Leste are susceptible to a pregnancy.14
Close birth spacing is an issue in the region, particularly in eight countries: in India, Jordan, Kyrgyz Republic, and Timor-Leste, more than 20% of women give birth within two years of a previous birth, and in Afghanistan, Pakistan, Tajikistan, and Yemen, the figure is 30% or higher. In fact, 1 in 10 women in these eight countries give birth in very short birth intervals: only 7 to 17 months since the previous birth.

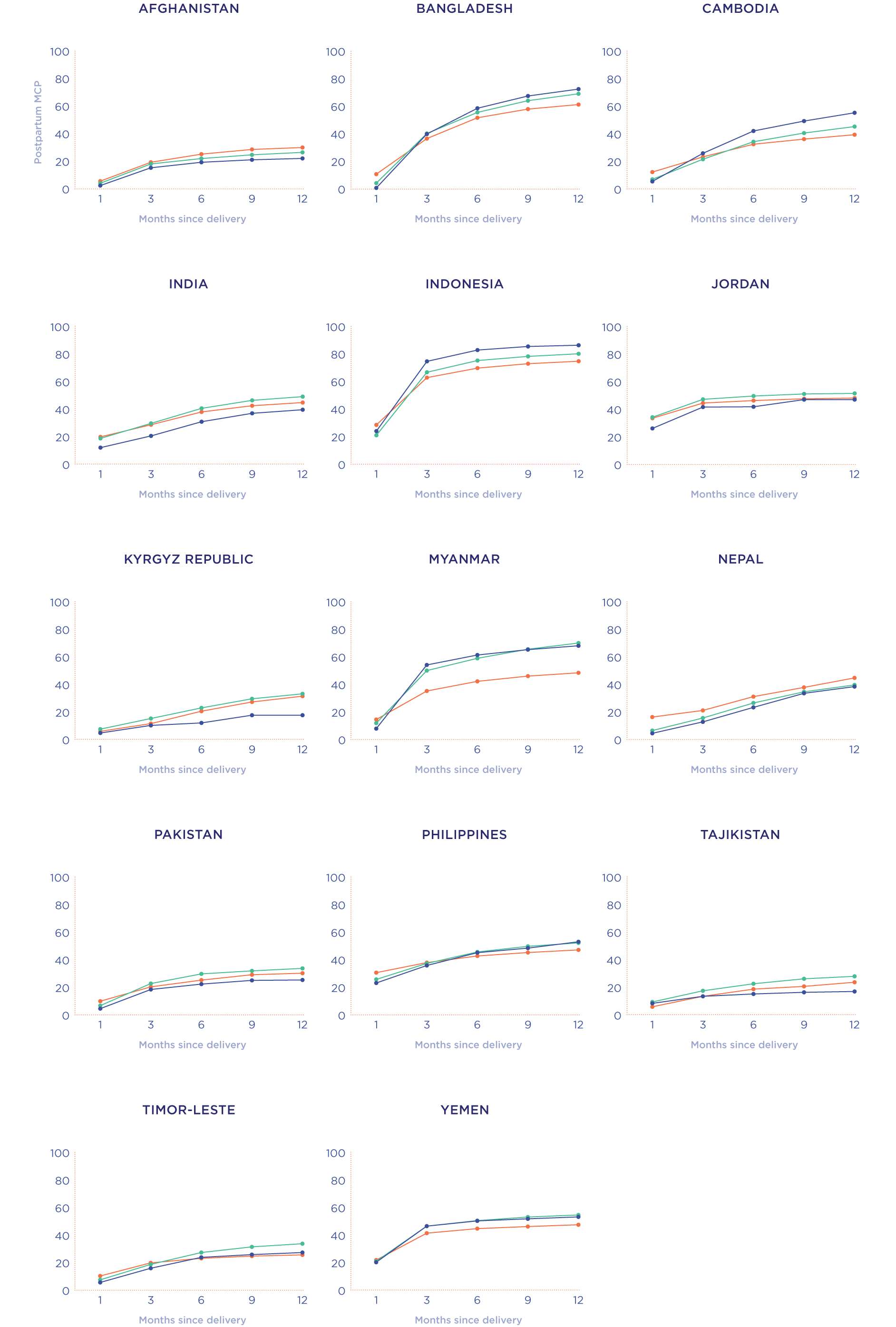
Facility Type: In all countries, women who deliver at home rather than in a facility (public or private) have the lowest MCP, although the gaps are not wide as they are in the ESA or NWCA regions. Furthermore, in all countries we reviewed (except Afghanistan), by 12 months postpartum there is no significant difference in MCP among women who delivered in a public facility versus a private facility. In Afghanistan there is about a 10 percentage point difference between women who delivered in a private facility versus a public facility (42.3% vs. 31.2%, respectively).
Age of Mother at Most Recent Birth: In seven countries — Afghanistan, India, Jordan, Kyrgyz Republic, Nepal, Pakistan, and Tajikistan — modern contraceptive uptake is lowest among the youngest mothers (under age 20). In two countries, Kyrgyz Republic and Tajikistan, the MCP gap between the youngest mothers and those aged 20-34 or 35-49 actually widens over time. The situation is reversed in Cambodia and Indonesia, where postpartum contraceptive uptake is lowest among the oldest mothers (those aged 35-49) and highest among the youngest (those under age 20).
Shore up any gaps in timely postnatal care. In stark contrast to ESA and NWCA, the AP region has a strong record on prompt postnatal care. In eight of the 11 countries with data on timing (Bangladesh, Cambodia, India, Indonesia, Jordan, Nepal, Pakistan, and Tajikistan), more than half of mothers receive a postnatal check within 4 hours of delivery.16 The chief outlier is Timor-Leste, where the majority of women do not receive a postnatal check until 41+ days after delivery or never. This is also the case for more than 20% of women in Myanmar, Nepal, and Pakistan.
Take advantage of the immediate postpartum window to offer contraception. In 10 of the 11 countries with data on timing (except Cambodia), current modern contraceptive use is higher for women who received their postnatal checks within 4 hours of delivery compared to women who received their postnatal checks at 41+ days or never. The contrast is most pronounced for women in Myanmar (63% vs. 46.4%) and the Philippines (51.7% vs. 36.3%). There is no difference in Cambodia.
Ensure that postnatal checks include counseling on birth spacing and family planning. Young or unmarried women should not be denied services. The latest DHS surveys in Cambodia, Nepal, and the Philippines include questions about the content of postnatal checks. The majority of women in Cambodia and the Philippines received information on family planning during their postnatal checks, but only about a quarter of women (25.4%) in Nepal received this information. The most recent Service Provision Assessment from Nepal (SPA 2021) shows a similar percentage, with 23.6% of postpartum women being counseled on family planning and 3.6% adopting a method. The youngest mothers in Nepal (those under age 20) are less likely to be counseled on family planning than older mothers (aged 20-49). Very few consultations (1% or less) included discussion of newborn care, breastfeeding practices, infant vaccinations, or family planning.17

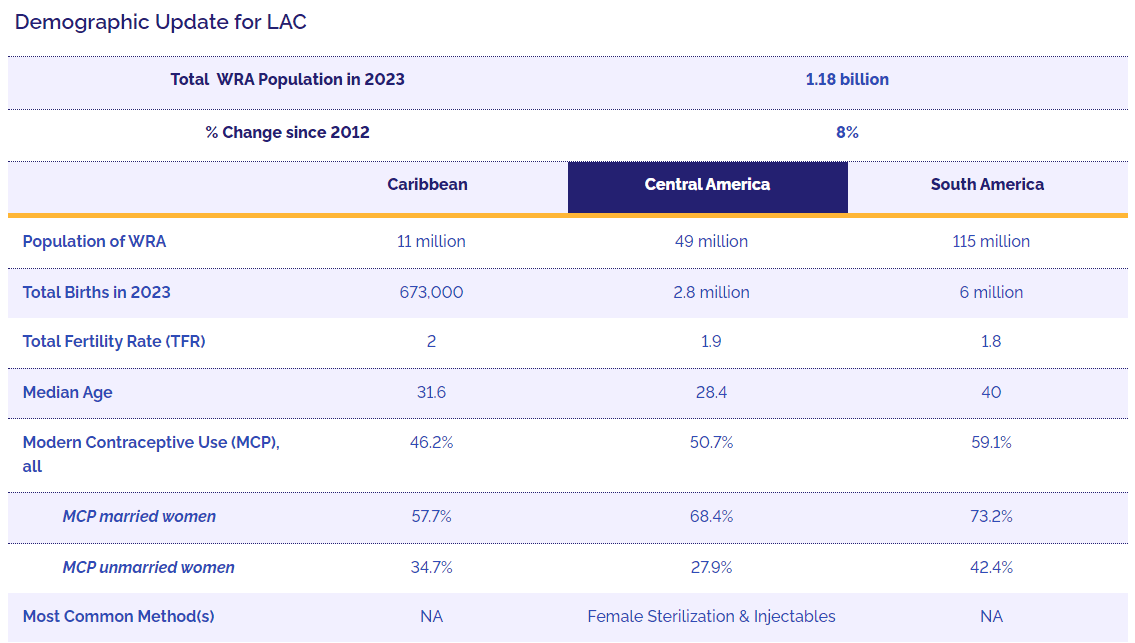
LAC differs from our other regions in a number of respects, with a population that is older and growing more slowly than those in Africa or Asia. The median age is 30.9, and the fertility rate in every subregion and in LAC as a whole is below replacement level.
The population of WRA grew by 7.9% between 2012 and 2023, from 162 million to 175 million. About 800,000 women reached reproductive age in the past year (2022 to 2023). The fastest growth is in Central America, where the population of WRA increased by 12% between 2012 and 2023.
Total WRA Population in 2023
1.18 billion
% Change since 2012
8%
Caribbean
Central America
South America
Population of WRA
11 million
49 million
115 million
Total Births in 2023
673,000
2.8 million
6 million
Total Fertility Rate (TFR)
2
1.9
1.8
Median Age
31.6
28.4
40
Modern Contraceptive Use (MCP), all
46.2%
50.7%
59.1%
MCP married women
57.7%
68.4%
73.2%
MCP unmarried women
34.7%
27.9%
42.4%
Most Common Method(s)
NA
Female Sterilization & Injectables
NA
Modern contraceptive use in the LAC region is high — higher than in most regions in Africa or Asia and Pacific. Estimates suggest that more than 70% of married women and more than 55% of all women were using modern contraception in 2023. Little recent data on sexual and reproductive health, however, are available for the region. Only five LAC countries have conducted a household survey with women of reproductive age since 2014 (Belize, Bolivia, El Salvador, Haiti, and Honduras), so few in-depth insights on the last decade of progress are available at national and subnational levels or with historically marginalized populations such as indigenous peoples and Afro-descendants. Some indicators do however suggest remaining SRHR challenges in the region.
While in much of the world the availability of newer contraceptive methods has resulted in shifts to long-acting reversible contraceptives, most LAC countries reported little use of these methods in their last reproductive health surveys.18 In three of the five LAC countries with surveys since 2015 — Belize, El Salvador, and Honduras — female sterilization was the most common method. Injectables were the most common method in Bolivia and Haiti, and the second-most common method in Belize, El Salvador, and Honduras. Implants and IUDs, which are widely used throughout Africa and Asia, have not emerged as commonly used methods in the LAC region. Usage of long-acting reversible contraceptives is low among the entire population, but appears to be lowest among poor, rural, uneducated, young, and indigenous women.
Another challenge in the LAC region is the high adolescent birth rate. The adolescent birth rate in the region is 53 births/1000 women aged 15-19, and is particularly high across most countries in Central and South America. What stands out in the LAC region is that the adolescent birth rate is higher than in comparable upper-middle income countries in other regions, and higher than in countries and regions with similarly high levels of contraceptive use. These differences may suggest barriers to young people’s SRHR, but again little in-depth data is available from recent surveys.
In order to better understand possible barriers to expanded method availability and meet the needs of young people and other populations, FP2020 will work with data partners to shine a light on the issues that hamper data collection and analysis. More broadly, FP2030’s work in the region will focus on calling attention to the remaining challenges, strengthening our engagement with civil society organizations and youth-led organizations, and gaining commitments from governments, donors, and technical partners to this unfinished agenda.
PHOTO BY Paula Bronstein/Getty Images/Images of Empowerment, Shutterstock, Shutterstock, Paula Bronstein/Getty Images/Images of Empowerment, Shutterstock

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}