
In the 2021 Measurement Report, we marked the transition from FP2020 to FP2030 with a broad overview of regional family planning data and trends in Africa, Asia & the Pacific, and Latin America & the Caribbean. In this year’s report we take a narrower approach, focusing on only one region—sub-Saharan Africa—and the 15 countries in that region that finalized their FP2030 commitments by August 2022. Six of the countries (Ethiopia, Madagascar, Mozambique, Rwanda, Tanzania, and Uganda) are in East & Southern Africa, and nine (Benin, Burkina Faso, Guinea, Mali, Mauritania, Niger, Nigeria, Senegal, and Togo) are in West Africa.
The 15 country commitments share many common priorities: improving service delivery for young people, increasing domestic financing, scaling up postpartum family planning, and strengthening supply chains. In this analysis we review regional and country-specific data trends in two of those priority areas—adolescent and youth contraceptive use and postpartum family planning—to explore how country commitments match up with opportunities to improve sexual and reproductive health outcomes. While some countries may be able to continue implementing their family planning programs as before, others may need to make adjustments to improve access for different populations.
The 15 commitment-making sub-Saharan African countries all have large and growing adolescent and youth populations. As these populations enter their reproductive years, demand for family planning services will continue to rise.
Young married women aged 15–24 rely on short-acting contraceptive methods such as injections and pills and obtain their methods from government facilities.
More than 1 in 10 women of reproductive age are postpartum in any given year, and the majority (except in Rwanda) are not using modern family planning, despite the importance of birth spacing for the health of the mother and newborn.
Most unmarried sexually active women aged 15–24 rely on condoms and obtain their contraceptive methods from private health sources. There is some evidence to indicate an increase in the use of long-acting methods (such as implants) among unmarried sexually active women in West Africa.
In most of the countries, more than 1 in 5 sexually active young women (aged 15–24) have an unmet need for contraception.



High-quality, comprehensive family planning services for adolescents and young people are crucial for improving sexual and reproductive health, reducing the risk of unwanted pregnancy and sexually transmitted diseases, keeping girls in school, and empowering young women to participate fully in society. The Family Planning High Impact Practices (HIPs) partnership identifies adolescent-responsive contraceptive services as a High Impact Practice with demonstrated effectiveness for increasing adolescent contraceptive use.
The population skews young in all 15 of the commitment-making countries we examined, with more than 1 in 5 women of reproductive age in their teens (aged 15–19). Thirteen of the countries (excluding Mauritania and Togo) have more than 1 million young women aged 15–24. Unmet need in this age group is high: In most of the countries, more than 1 in 5 sexually active young women have an unmet need for contraception. Appropriately, all 15 country commitments prioritize adolescent and youth services.
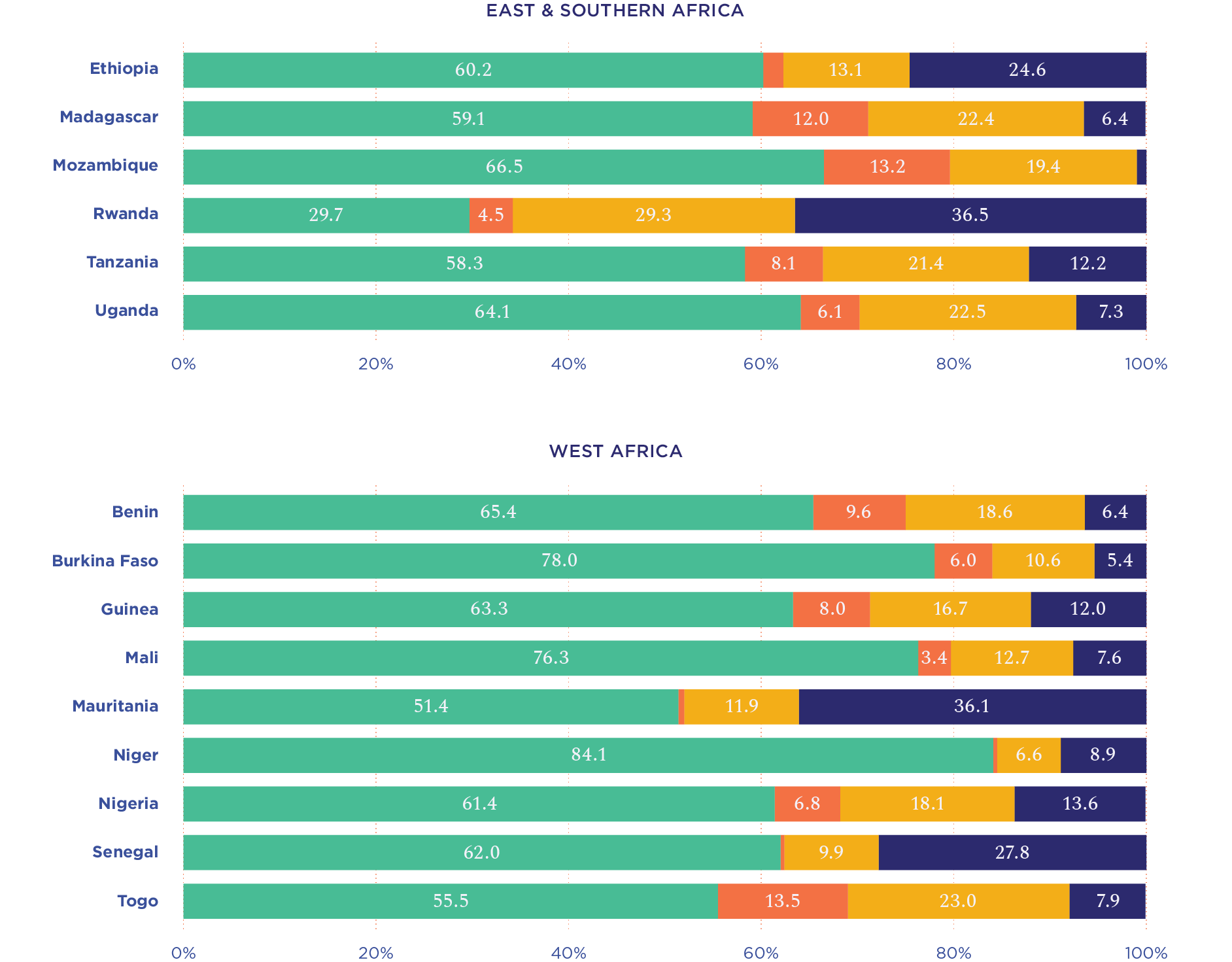
On average, women in these countries first have sex around age 17.5, get married for the first time around age 19, and give birth for the first time around age 20. Since most women do not start having sex until after age 17, the majority of girls in the 15–19 age group have never had sex (Figure 4). However, as they enter the next age group (20–24), virtually all have started engaging in sexual activity (Figure 5).
The gap between first sex and first birth is typically about 2.5 years. But differences in marriage patterns across countries determine how much of this gap takes place within or outside of marriage. In Rwanda, for example, the average age of first sex is 20.7, with first marriage following at age 22.8 and first birth at 23. At the opposite end of the spectrum is Niger, where the average age of first marriage is 15.7, with first sex following at age 15.9 and first birth at age 18.6. (Niger is the only country in our sample where the start of sexual activity typically occurs for young women after they are married.)
To ensure that young women are able to make informed decisions about contraceptive use before they get married or become sexually active, programs should tailor messages to reach girls as soon as they enter their reproductive years. Programs should also be responsive to the different needs of sub-populations. One group that is easily overlooked is unmarried young women who have not recently been sexually active, with recency defined as being within the past 30 days (yellow bars in Figures 4 and 5). This group is in fact a larger proportion of the population than unmarried young women with recent sexual activity (orange bars). Programs will need to take into consideration the life experiences and specific needs of this group and other sub-populations to ensure that outreach strategies are appropriate.
Contraceptive use among married and unmarried sexually active women aged 15–24 is generally higher in East & Southern Africa than in West Africa (Figure 6). The difference is especially pronounced among young married women: In East & Southern Africa, the modern contraceptive prevalence, or MCP, rate for married women aged 15–24 ranges from 21.4% in Mozambique to 61.1% in Rwanda; in West Africa, it ranges from 6.4% in Nigeria to 30.2% in Burkina Faso.
Unmet need for unmarried sexually active young women is also generally higher in West Africa, especially for those aged 15–19. In three countries (Benin, Mali, and Nigeria), over 50% of unmarried sexually active women aged 15–24 have an unmet need for family planning.

Nigeria’s high population means that even small percentages translate into large absolute numbers. At 14.9%, Nigeria’s percentage of young married women with unmet need for family planning is not as high as in the other West African countries we examined. But because of population size, that 14.9% equates to 1.3 million women—by far the most of any country in our sample.
By the same token, Nigeria’s 6.4% MCP among married women aged 15–24 is the lowest of all 15 countries we analyzed. But that works out to approximately 550,000 users—more than four times the number in Rwanda, which has the highest MCP for young married women of any country in our study (61.1%).
Regional differences in method choice
Different youth populations in the two subregions rely on various modern methods (Figures 7 and 8). Modern contraceptive method choice generally tracks with marital status (married versus unmarried and sexually active) rather than age cohort (15–19 versus 20–24), so the figures show disaggregation by marital status only.
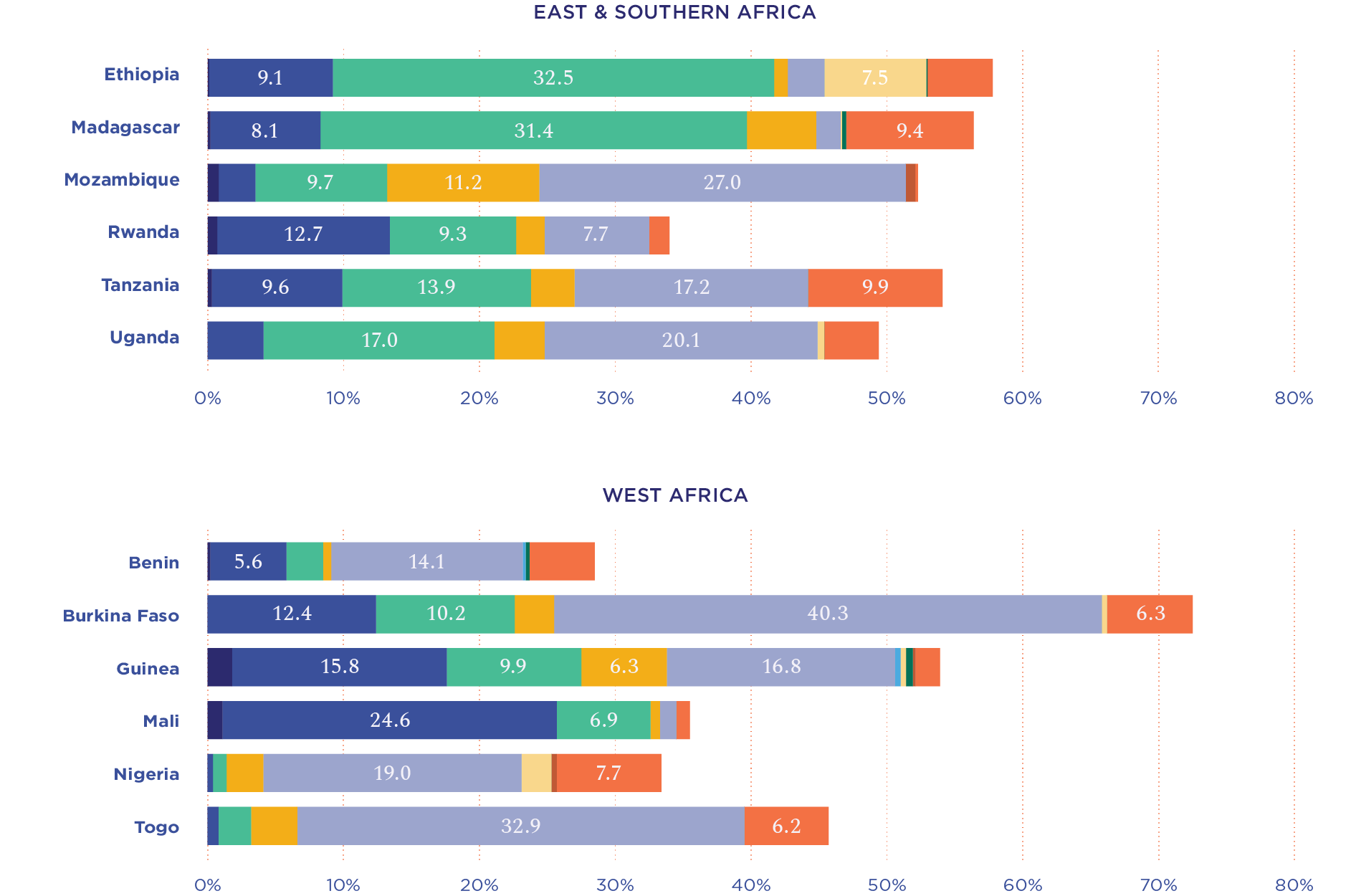
Even though married women aged 15–24 overwhelmingly use short-acting contraceptive methods in both East & Southern Africa and West Africa, there are regional and country-specific differences (Figure 7). Injections are more popular in East & Southern Africa, making up over 50% of the modern method mix for married women aged 15–24 in Ethiopia, Madagascar, and Uganda. West African countries have more varied method use, with less dominance by a single method. Mauritania is the only country where pills were used by over half the married modern contraceptive users aged 15–24. In Guinea, where contraceptive use is low among married women, most of the married women aged 15–24 who are using a modern contraceptive method use the lactational amenorrhea method (LAM).
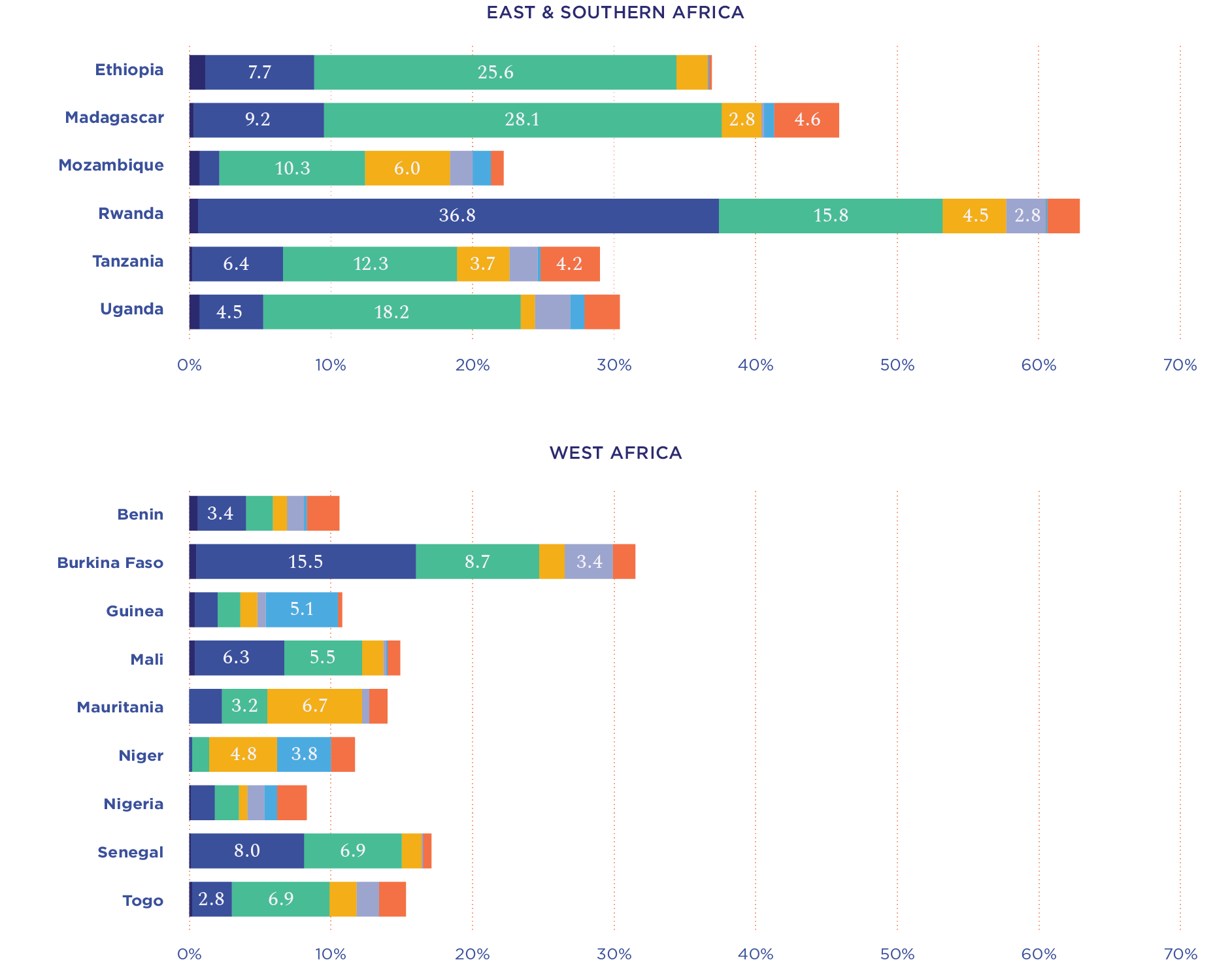
Among unmarried sexually active women aged 15–24, condom use is the leading contraceptive method in the majority of countries (Figure 8). In East & Southern Africa, injections are also very popular and are the leading method in Ethiopia and Madagascar.
Unmarried sexually active young women in West Africa use long-acting reversible methods, especially implants, at a higher rate than women in East & Southern Africa. Between 2012 and 2018, the use of implants in Benin, Guinea, and Mali more than doubled among this population, and today more than 1 in 5 unmarried sexually active contraceptive users in these countries are using implants. Additionally, among unmarried sexually active young women in Burkina Faso, self-injections are more popular with the 15–19 age group (7.3%) than the 20–24 age group (3.4%), however, it should be noted that the sample size for both groups is very small.
Regional- and country-level differences in contraceptive method use can have significant implications for family planning programs, including the types of counseling and service delivery that should be offered for various youth populations. Recent method use trends among unmarried sexually active young women in Benin, Burkina Faso, Guinea, and Mali, for example, might signal that this population would opt to use methods other than condoms if those methods were readily available and accessible.
The different contraceptive method use patterns between married and unmarried young women may be due to where they are obtaining their methods. In all countries in our sample, most married women aged 15–24 obtained their most recent modern contraceptive method from a government health facility. Most unmarried sexually active young women aged 15–19 in Benin, Mozambique, Nigeria, Tanzania, Togo, and Uganda obtained their methods from private sources such as shops and pharmacies; these are also countries where condom use makes up over 50% of the modern method mix for unmarried sexually active women aged 15–19. Greater reliance on the private sector by unmarried young women, especially those aged 15–19, might indicate a lack of public sector reach with this segment of the population or poor quality of service provision for the youngest women. It is important for countries to evaluate their method mix as well as the source of those methods to understand if the family planning program is meeting the needs of all young people—and where there might be bottlenecks.
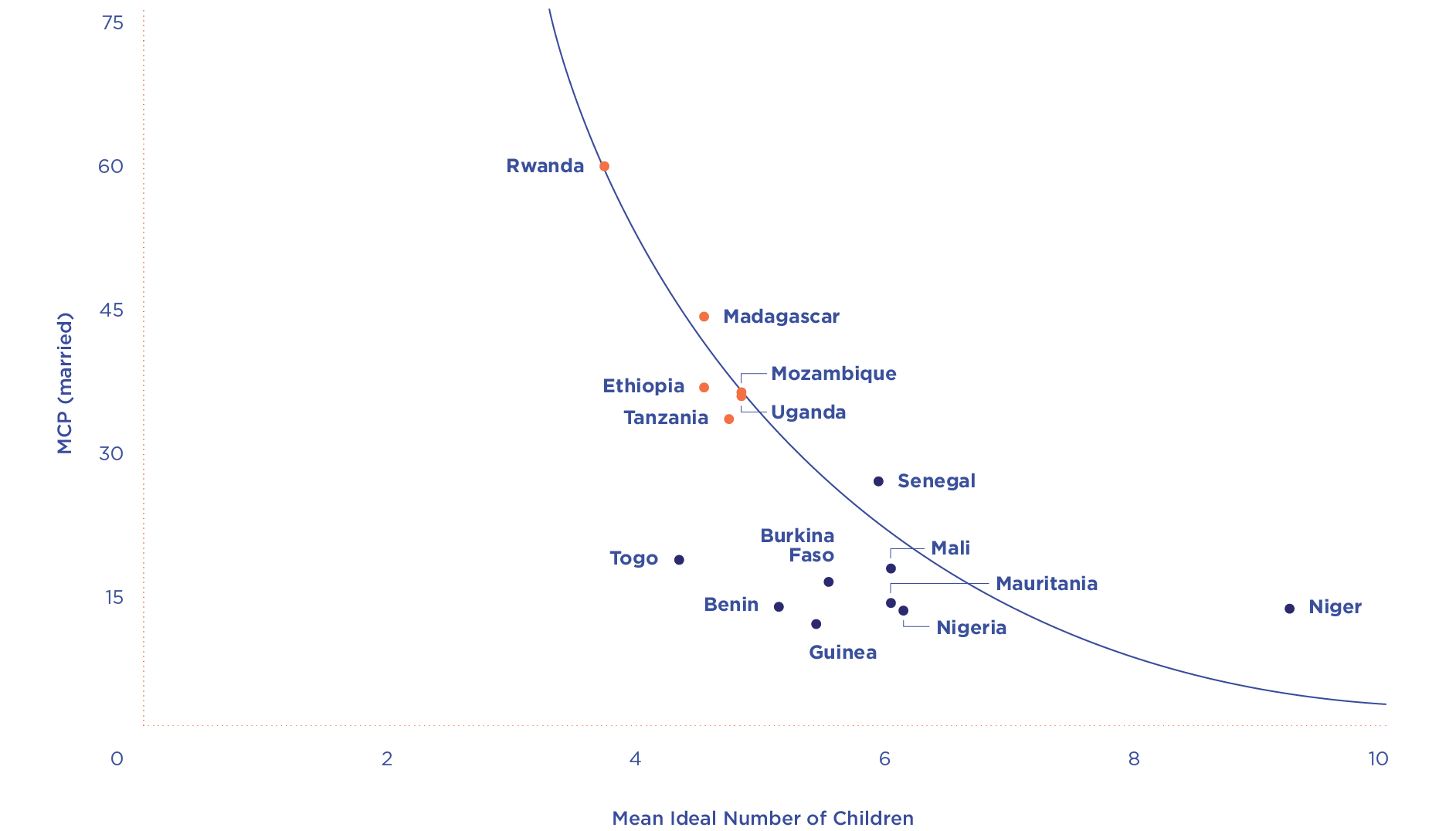
Another common priority among the commitment-making countries in sub-Saharan Africa is postpartum family planning (PPFP), another High Impact Practice with demonstrable effect on contraceptive use across many settings. PPFP saves the lives of mothers, newborns, and children by providing contraceptive counseling and services during antenatal care, labor and delivery, and the postpartum period. Thirteen of the country commitments we analyzed emphasize PPFP strengthening or expansion. To evaluate the potential increase in demand for postpartum contraception, we examine the “demand curve” of maximum modern contraceptive prevalence in these countries (Figure 9) as well as the percentage of women who are postpartum at any given time.) as well as the percentage of women who are postpartum at any given time.
The demand curve was developed by Track20 to represent the likely maximum MCP that can be reached in a country given the level of demand. The curve is created by fitting an exponential curve to the maximum of all available DHS survey data on MCP and ideal number of children, an indicator that represents a broad range of social and cultural norms that influence the motivation to use, or not use, contraception.
In all 15 countries for which we have analyzed commitments, the mean ideal number of children is high, ranging from 3.7 in Rwanda to 9.2 in Niger. It is generally higher among West African countries than East & Southern African countries. The gap between where a country sits on the graph and the curve is called the “potential use gap” and indicates where there is room for increased uptake of family planning. The larger the preferred family size, the more likely women are to use family planning to space births rather than limit them.
In Togo, for example, current modern contraceptive prevalence for married women is 17.3% and the mean ideal number of children of 4.3. The gap between the current MCP and the curve is about 25 percentage points. That should be considered the maximum increase in MCP possible for Togo given women’s current fertility desires.
The closer a country is to the curve, the less opportunity there is for modern contraceptive prevalence to increase and the more slowly MCP will grow. For countries sitting right on the curve or close to it, future growth in MCP may not be possible unless there are further changes in demand. This can happen if social norms change and women begin preferring smaller families. If the mean ideal number of children decreases, the demand for modern contraception will increase as more women seek to prevent unintended pregnancy.
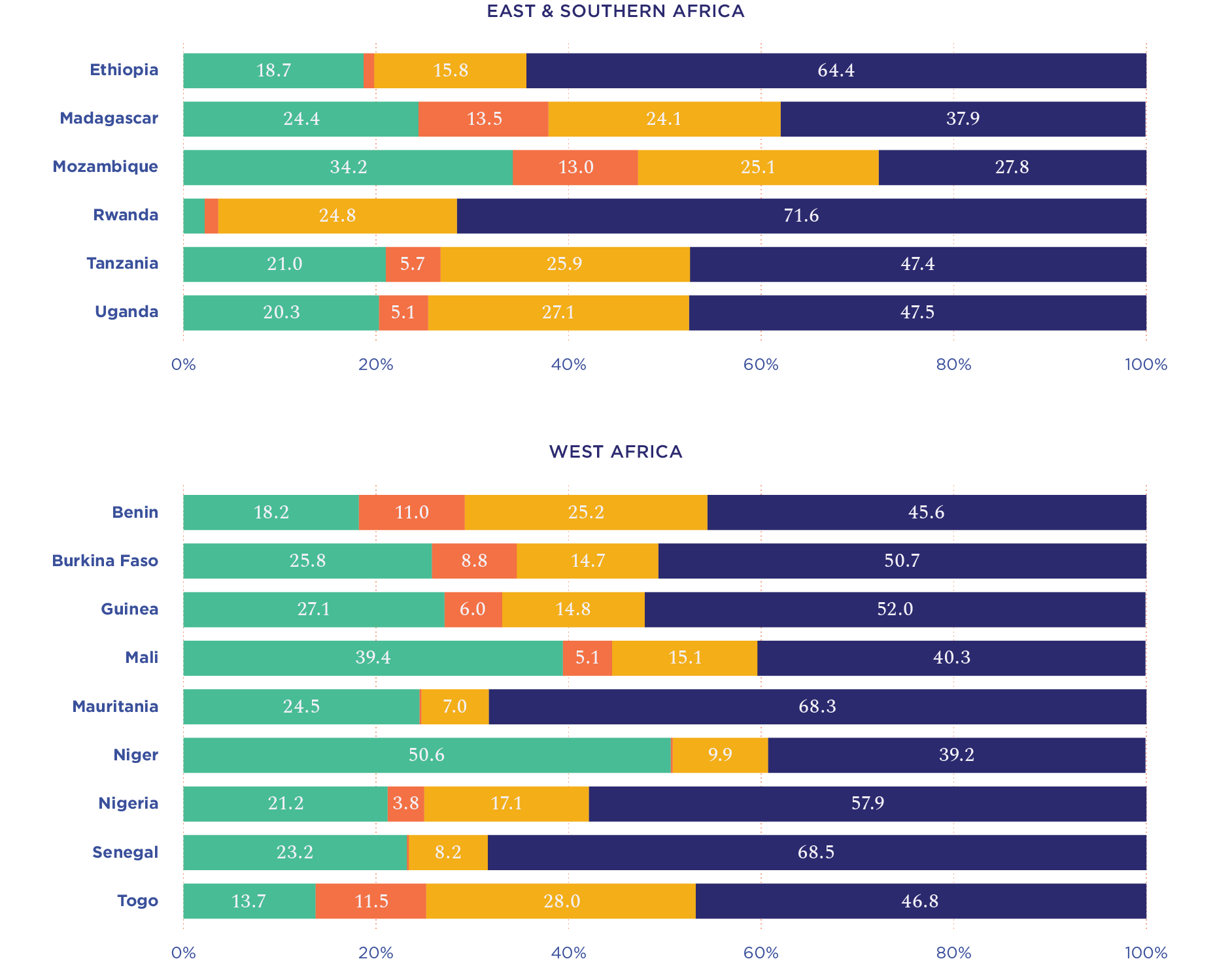
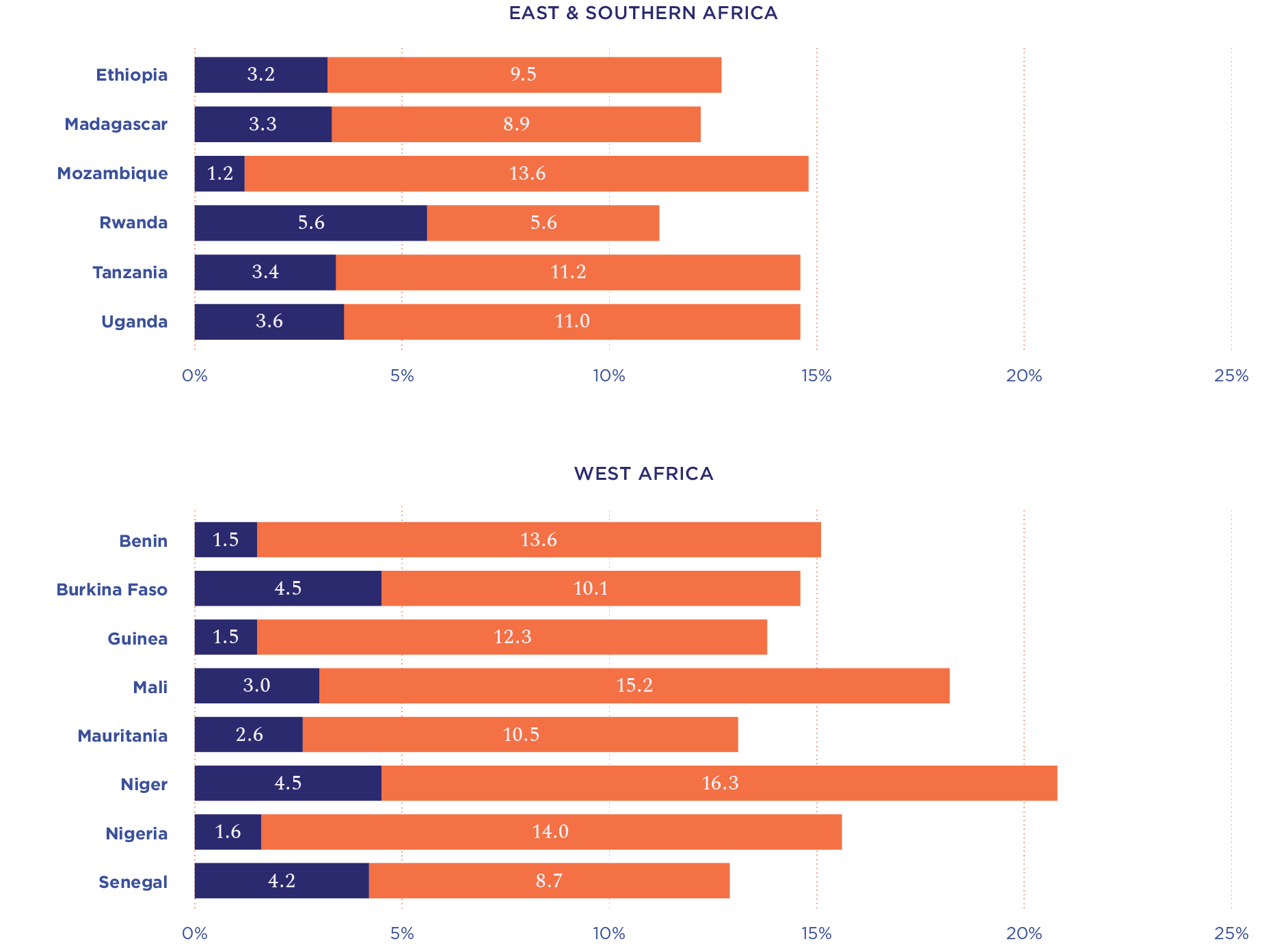
Given that ideal family size preferences are large in these 15 countries, it is important to review the current use of postpartum family planning. A preference for more children in West Africa is reflected in the higher proportion of postpartum women in this subregion than in East & Southern Africa (Figure 10). Across Mali, Niger, and Nigeria, over 15% of women of reproductive age are postpartum in any given year, and most of these women are not using modern contraception for birth spacing or limiting.
The East & Southern African countries in our sample have a smaller proportion of postpartum women (less than 15% at any given time). Except in Rwanda, fewer than half of these postpartum women are using modern contraception. While countries cannot expect all postpartum women to use family planning, there is nevertheless a significant opportunity to increase contraceptive choice and reduce maternal and newborn mortality through improved PPFP counseling and service delivery.
Since 2015, the Rwanda Ministry of Health has worked with global partners such as the Maternal and Child Survival Program of the U.S. Agency for International Development (USAID) to expand postpartum family planning (PPFP) services.
The scale-up of PPFP interventions resulted in tremendous gains, with modern PPFP use at six months increasing from 38% in 2014 to 50% in 2019. Today, around 50% of postpartum women in Rwanda are using a modern method of contraception.
These results also suggest that while modern contraceptive use among postpartum women can significantly increase if family planning programs improve interventions, not all postpartum women will opt to use modern contraception.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}