Until women are able to decide for themselves what happens to their own bodies, gender equality will remain an unreachable dream. Access to contraception is the critical factor that unlocks a world of possibilities for women and girls: finishing school, pursuing a career, planning for and starting healthy families, and participating fully as equal members of society. Voluntary, rights-based family planning is essential for progress on gender equality.
At the same time, a keen understanding of gender norms and constraints is essential for family planning programs to succeed. Harmful gender dynamics are some of the most persistent barriers to contraceptive use. Child marriage, reproductive coercion, misinformation, and stigma all prevent individuals from exercising reproductive agency and accessing family planning services. Gender discrimination in the health workforce and the absence of women’s voices in program design lead to inadequate services that do not truly meet people’s needs. Antiquated policies and lack of funding for women’s health result in fewer contraceptive choices, increased likelihood of stockouts, and service quality issues — which in turn translate directly into fewer people using and benefiting from contraception.


Gender has been a dominant focus throughout the past year of FP2030. At the 67th Commission on the Status of Women in March 2023, we launched the FP2030 Gender Strategy, a set of principles and approaches designed to make FP2030 more effective, more strategic, and more representative of women, girls, and all people. At the International Maternal and Newborn Health Conference in May, we hosted Stronger Together, bringing together two critical areas of care—maternal and newborn health and family planning—to discuss how an integrated approach can save the lives of both mothers and newborns while also increasing the use of family planning post-partum. At Women Deliver in July, we hosted Equity Means Everyone: Expanding the family planning movement to achieve the SDGs, focused on how the movement for voluntary family planning is intrinsically tied to the broader movement for human rights. That was also the theme in our two Women Deliver pre-conferences, Girls Deliver and Gender and the Climate Crisis. And at COP28 in November we were able to deepen our relationships with population, health, and environment experts. Women are uniquely vulnerable to climate change and also uniquely positioned to take climate action; their needs must be part of the equation when developing adaptive strategies.
The links between family planning and gender equality are the central theme of this year’s Measurement Report. Our data set covers 85 countries, including for the first time Botswana and Namibia, two middle-income countries that have now made commitments to FP2030, and Jordan, which has moved into the lower-middle income category.1 The report also reflects the impact of the decentralized FP2030 Global Support Network, with input from all five Regional Hubs: Asia and Pacific; East and Southern Africa; North, West, and Central Africa; and Latin America and the Caribbean.
GLOBAL TRENDS finds the family planning movement at a pivotal moment, with progress in contraceptive use juxtaposed against diminishing international aid and shifting political priorities. The number of women using modern contraception has grown by 92 million since the outset of this partnership in 2012, and modern contraceptive prevalence has increased to 35.2%. Countries with the lowest levels of contraceptive use a dozen years ago are now in the midst of a family planning boom, other countries have successfully reinvigorated aging programs, and highly effective, long-acting implants have become the method of choice across much of Africa.
But there are also warning signs ahead. The population of contraceptive users is continuing to rise, but global funding for family planning is stagnant. Contraceptive prevalence in some countries is plateauing at low levels despite a high percentage of women still wanting to limit or space births. Other countries are moving into a phase where continued progress will depend on serious investment in transforming gender norms and scaling up high impact practices.

REGIONAL PROFILES explores one of those high impact practices in depth: postpartum family planning. In 2023 there were 59 million unintended births in low- and lower-middle income countries, and 80% of all births to teenage mothers occur in these countries. The FP2030 Regional Hubs specifically requested a study of contraceptive uptake in the postpartum period, one of the most critical moments in a woman’s life. We review the data for each region in the context of gender norms and explore the possible impact of age, marital status, and place of delivery. Our analysis reveals the signal importance of prompt postnatal checks and points to serious gaps in existing postnatal care.

FINANCE reports on resource flows for family planning in 2022, and has been revamped this year to provide better insight into how FP2030 and other data partners work together to track expenditures for sexual and reproductive health. We explain how family planning is funded by three types of expenditures: domestic government resources, donor financing, and consumer spending.
While our most recent estimates for domestic government spending (US1.68 billion) and consumer spending (US$710 million) are on par with earlier estimates, donor government contributions are on a downward trend. The estimated funding from donor governments in 2022 (US$1.35 billion) is 10% lower than the previous year and 15% below the peak level in 2019. Donor government funding is now at its lowest level since 2015 — yet the population of women of reproductive age has increased by 20% since the outset of this partnership in 2012.
If donor funding continues to stagnate or shrink, it could imperil the achievement of country goals for family planning as well as the Sustainable Development Goals. Donor financing is just one piece of the total resource package, but it plays an essential role in assisting countries to expand and strengthen their family planning programs, secure the supply of commodities, and incorporate higher priced contraceptives into the method mix.
The findings in this report suggest a straightforward agenda for the family planning community to rally around:
Invest to ensure that funding levels match the size of the current and projected user base. The number of women of reproductive age has grown by 20% since 2012 and is continuing to rise. Countries and their donor partners need to develop long-range resource plans to ensure that family planning programs are appropriately funded for the foreseeable future. What level of expenditure is needed to serve a growing population, both today and in years to come? What additional expenditures are needed to expand and strengthen services in accordance with country goals? These projections should guide resource planning for countries, donors, and the global family planning sector.
Invest to support and expand implant access throughout the world. Implants have proven hugely popular in Africa and may be one of the keys to achieving long-term improvements in contraceptive prevalence. But they remain expensive and must be subsidized by the international community. We need to maintain implant access where it already exists and expand access to regions and demographic groups that have been left behind.
Invest in postpartum family planning (and other high impact practices). Postpartum family planning is a key intervention that has been proven to save the lives of mothers and newborns and increase the uptake of contraception. We need to close the gaps in the continuum of care and ensure that every mother receives prompt postnatal care with counseling on family planning that is tailored to her needs. Young or unmarried women should not be denied services, and the quality of care should be at the same level regardless of facility.
Invest in gender-transformative approaches to family planning to shift norms and advance gender equality. This is long-range work and requires real commitment to social change, but it is essential if we are to achieve lasting progress in rights-based family planning. Gender-transformative programs and interventions are designed to actively challenge gender norms, address power inequities between men and women, and promote women’s empowerment — in everything from making decisions about their own reproductive lives to exercising political leadership in their communities.
Adopting a gender-transformative lens also has implications for family planning metrics. Measurements of success must go beyond modern contraceptive prevalence to capture degrees of reproductive empowerment: the ability of individuals to make informed decisions about their reproductive lives and achieve their reproductive goals. From a technical standpoint this is a complex measurement challenge, but one on which FP2030 and other family planning data partners are already embarked (see Areas of Future Work).
As the global push for gender equality gains strength, FP2030 affirms the central importance of rights-based, gender-transformative family planning. Contraception is fundamentally about bodily autonomy, and the movement to make modern contraceptive available to all people is part and parcel of the movement for human rights, dignity, and equality. FP2030 is committed to advocating, supporting, and implementing that agenda, and to developing better data tools that truly reflect the lived experiences of women and girls.
The language throughout this report refers to women or women and girls, which should be understood to include women and girls of reproductive age (15-49). But not all individuals who become pregnant are women and girls; transgender men and nonbinary people can and do become pregnant. However, the data used in this report overwhelmingly come from surveys and studies that identify participants as women or girls, and to extend the conclusions from those data to include gender-diverse people could result in inaccuracies or even the erasure of concerns specific to sexual minorities (UNFPA, State of World Population 2022). Therefore, we calculate contraceptive use and measure contraceptive prevalence based on women and girls using these methods, while acknowledging that some users may identify as transgender men or nonbinary people.
We also acknowledge that the data used in this report may not represent certain marginalized groups, such as people with disabilities, migrants, refugees, and ethnic minorities for whom data is not collected systematically through household surveys or other regular data systems.
In addition, the data from countries with on-going crises may not reflect the impact of the crises on family planning services and contraceptive use.
Data systems may not capture data for all groups nor for rapidly changing situations, but FP2030 is committed to advancing SRHR for all and looks for insights on challenges to access beyond just the data featured in this report.
After a decade of progress during the FP2020 partnership and resilience in the face of the global COVID-19 pandemic, the global family planning movement faces new challenges. Contraceptive use is continuing to grow and programs are expanding in many countries, but data suggest plateauing levels of overseas development aid. Geopolitical conflicts in Ukraine and the Middle East are diverting development assistance and challenging global cooperation. And the global movement to deny sexual and reproductive rights, particularly to adolescents and LGBTI people, has been bolstered by the United States Supreme Court’s overturning of the right to abortion. Together these challenges suggest that the family planning field is at an inflection point. Further progress in family planning is not guaranteed, and there are warning signs emerging from country, regional, and global data.
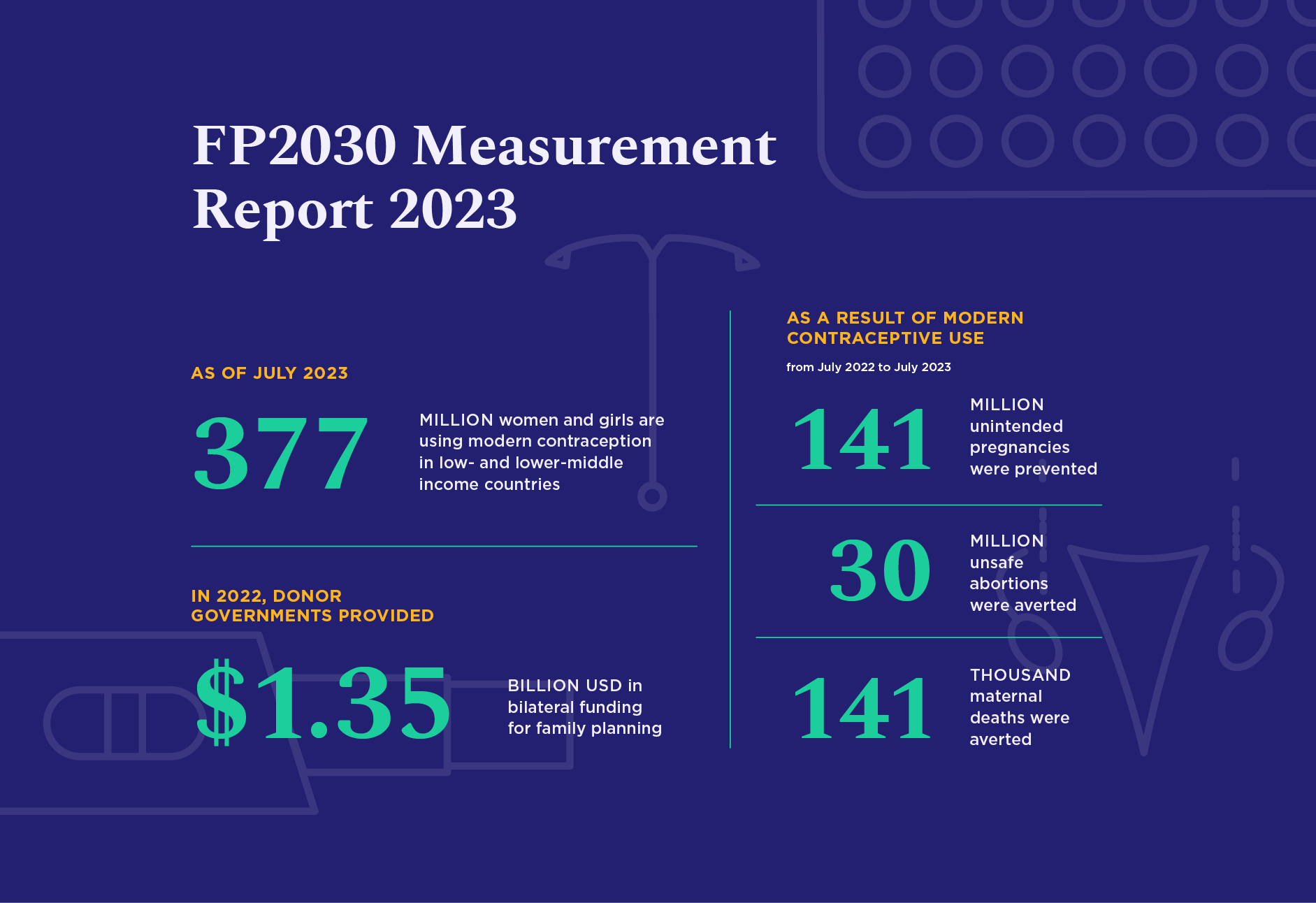
Despite these challenges, this year’s data illustrate the continued momentum of contraceptive growth and access to contraceptive services in many countries. There are just over one billion women of reproductive age (15-49) across the 85 reporting countries, and at the mid-point of 2023 an estimated 377 million of those women were using a modern method of contraception (Figure 1). Their use of modern contraception averted 141 million unintended pregnancies, 30 million unsafe abortions, and 141,000 maternal deaths in the last year alone.
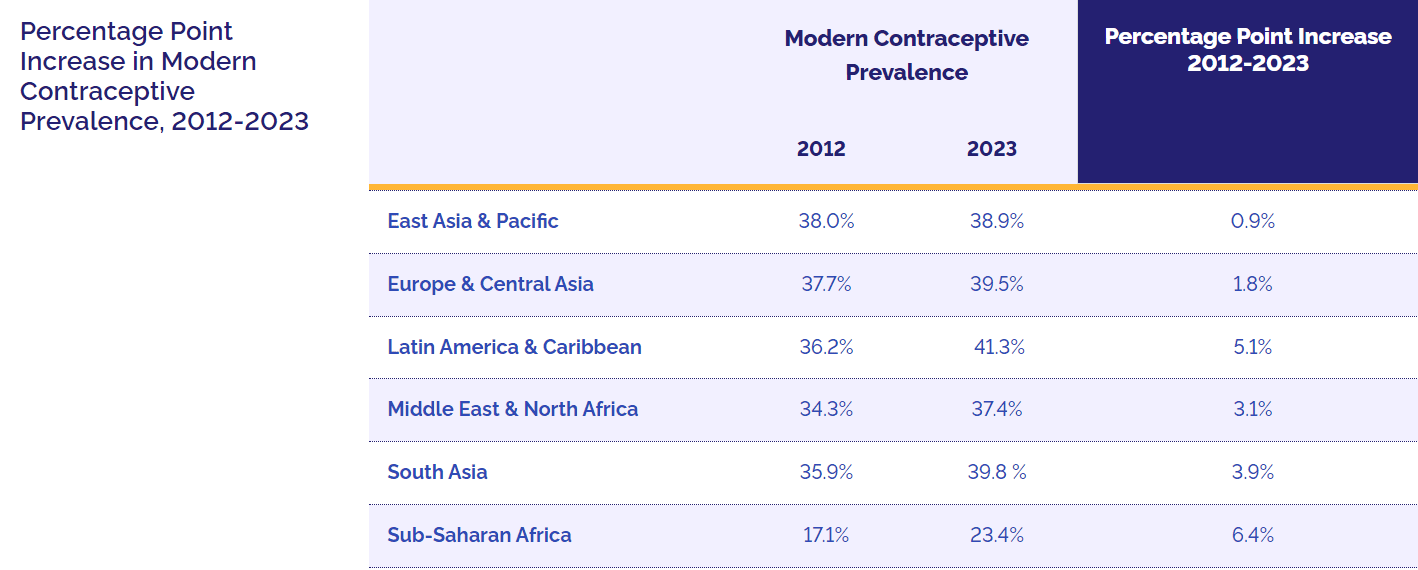
Modern Contraceptive Prevalence
Percentage Point Increase 2012-2023
2012
2023
East Asia & Pacific
38.0%
38.9%
0.9%
Europe & Central Asia
37.7%
39.5%
1.8%
Latin America & Caribbean
36.2%
41.3%
5.1%
Middle East & North Africa
34.3%
37.4%
3.1%
South Asia
35.9%
39.8 %
3.9%
Sub-Saharan Africa
17.1%
23.4%
6.4%
Another way to visualize growth is by looking at the average annual increase in MCP, both by region and by country (Figure 2). The average rise in MCP across all regions is 0.3% each year. But the fastest-growing regions (Western Africa and Eastern & Southern Africa) are moving at twice that rate. And in six countries — Burkina Faso, Malawi, Mozambique, Madagascar, Sierra Leone, and Uganda — MCP has risen by more than 1 percentage point per year since 2012. These are remarkable achievements, especially amidst the challenges of stagnant funding and the disruptions of the COVID-19 pandemic.
A deeper dive into the data reveals additional success stories:
Impressive changes in MCP in low prevalence countries. Many of the countries that were at or near the bottom of the S-Curve of contraceptive growth in 2012 have seen modern contraceptive use increase by large percentages; today they are in the middle phase of the S-curve, where rapid progress is possible.
This pattern is especially prominent in West African countries, including Benin, Burkina Faso, Côte d’Ivoire, DR Congo, Mali, Senegal, and Togo. Capitalizing on this potential will require continued commitment to supply-side factors — political support, funding, commodity availability, high impact practices — and increasing attention to the social and gender-based barriers that limit demand.
Growth in MCP past demand constraints. The Demand Curve of maximum contraceptive prevalence was developed by Track20 to model the likely maximum MCP that can be reached in a country given the existing level of demand for family planning. For countries that are near or above the curve, demand is a constraint: MCP probably cannot rise without changes in social norms and an increase in demand. Uganda and Zambia are two countries that have successfully grown past their demand constraints, registering large gains in MCP despite the theoretical limits. That suggests these countries are experiencing a real upward change in demand, possibly driven by shifting attitudes to contraception and more appealing method choices.
Increasing availability and popularity of implants. In 2012 there was only one country (Burkina Faso) in which implants were the most commonly used method of modern contraception. Today implants are the most commonly used method in 11 countries and the second most commonly used method in another 16 countries. This startling transformation is the result of the Implant Access Program, a public-private partnership that halved the price of contraceptive implants in FP2020 countries through volume guarantees. The program also trained providers in insertion and removal and cultivated awareness of long-acting reversible contraceptives (LARCs) at the community level. Implants have proven hugely popular and may be one of the keys to achieving long-term improvements in contraceptive prevalence — assuming that financial support continues.2
This year’s data also suggest that continued progress over the next several years is far from guaranteed. Warning signs are emerging that the road ahead will require more resources, sharper strategies, and deeper commitments:
Population of contraceptive users outstripping funding. As we saw above, the population of women of reproductive age has increased by 20% since 2012, and the number of contraceptive users has grown by 92 million. Yet donor government financing is trending downward, and is now at its lowest level since 2015 (see Finance). Donor financing is an essential component of the total resource package for family planning, alongside domestic government expenditures and consumer spending. If donor aid continues to shrink, it could become difficult in some countries to maintain the existing base of contraceptive users and almost impossible to expand it.
The stagnation in funding is especially problematic when it comes to donor-dependent methods like contraceptive implants. Implants are an important addition to the method mix, and should be made available to all potential users in every geographic region. But they are a relatively expensive method and donor subsidies are essential.
Countries plateauing in their progress. During the COVID-19 pandemic national demographic and health surveys were postponed, but after the pandemic many of these surveys were resumed. Since 2021 we have had 12 new country surveys to analyze, revealing that progress in some countries appears to have stalled. Honduras, Nigeria, Pakistan, and Tanzania are all examples of countries where MCP has plateaued or grown much more slowly than previously estimated. The reasons for this are different for each country, and may include a variety of factors: political challenges, funding issues, service or commodity problems, and entrenched gender norms that interfere with demand. (In some cases the reasons may be completely outside the purview of the family planning program; in Nepal, for example, MCP has barely budged since 2012, but Nepal is also experiencing significant male out-migration, so women have less need for contraception.) In any event, progress in expanding family planning is not assured without attention to the factors that may be constraining growth.
Impending slow-downs in formerly low prevalence countries. The fast-growing countries that have moved from the bottom of the S-curve to the middle are beginning to approach levels where further gains may not be possible without a change in strategy. Most of these countries will need to invest in social behavior change and communication projects to address existing gender norms and limitations on women’s decision-making power. They will also need to scale up high impact practices such as post-pregnancy family planning (postpartum and post-abortion family planning), which have the potential to reach women and girls at some of the most critical points in their lives.
This year’s Measurement Report covers 85 countries: the 82 countries classified as low- or lower-middle income in 2020; new commitment makers Botswana and Namibia, both middle-income countries; and Jordan, which moved down into the lower-middle income category on the World Bank’s updated country list released in July 2023.3 We recognize that our current criteria for inclusion in the Measurement Report excludes a large number of countries in Asia and Latin America and the Caribbean, and we will continue to assess the geographic scope of the report over the coming years of the partnership.
In addition to reporting on more countries than ever before, this year’s Measurement Report — along with a new dashboard and data resources — provides more insights on contraceptive use, adolescent and youth sexual and reproductive health, and finance trends than any previous FP2030 Measurement Report. Based directly on feedback from FP2030 focal points, country monitoring and evaluation officers, and civil society and youth advocates, FP2030 continues to develop new resources and provide additional visibility into data. Specific changes in this year’s dataset include new detail on country governments’ domestic expenditures, including spend on staff, commodities, and other components of the family planning program. In addition, FP2030 is now publishing trend data on domestic expenditures starting with 2020. Each of these advancements is due to the work of Avenir Health’s Track20 Project on annual Family Planning Spending Assessments (FPSAs), which have used a consistent methodology and process to support governments to track their FP expenditures over the last several years.

Also new to this year’s report is a renewed focus on improving the reporting of family planning decision-making, which contributes to reporting for the SDG indicator 5.3.1 on gender and decision–making. This indicator is meant to capture the extent to which women are engaged in the decision to use or not use contraception. This year’s report reflects a change decided upon by FP2030’s PME Working Group, and moves from reporting on whether women made a decision alone or jointly with their husband, to separating out those women who report that they do in fact make the decision alone.
Data and measurement advancement remain a critical aspect of FP2030’s strategy. In addition to improving data availability, we are also working to advance an FP2030 Measurement Agenda to address ongoing challenges: measuring quality of care (including clients’ experience of care), assessing autonomy and empowerment, capturing the influence of gender norms on family planning, and monitoring the scale-up of high impact practices.
In 2024, in collaboration with partners such as the PME Working Group, the Momentum Knowledge Accelerator Project, Performance Monitoring for Action (PMA), Track20, and the Post-Partum and Post-Abortion Family Planning Steering Committee, we are embarking on a Measurement Advancement Convening Series. This series of consultations is designed to foster more inclusive participation in the global family planning measurement agenda, drawing particularly on country experts and stakeholders across Africa, Asia, and Latin America and the Caribbean. The goal is to develop a locally-driven program of action to identify priorities, resolve longstanding challenges, improve existing measures, and create new indicators.
PHOTO BY Yagazie Emezi/Getty Images/Images of Empowerment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}